
Global Neonatal & Children's Health 2
Session: Global Neonatal & Children's Health 2
 photo")
Christina E. Stiles, MD (she/her/hers)
Resident Physician
UCSF Benioff Children's Hospital Oakland
Emeryville, California, United States
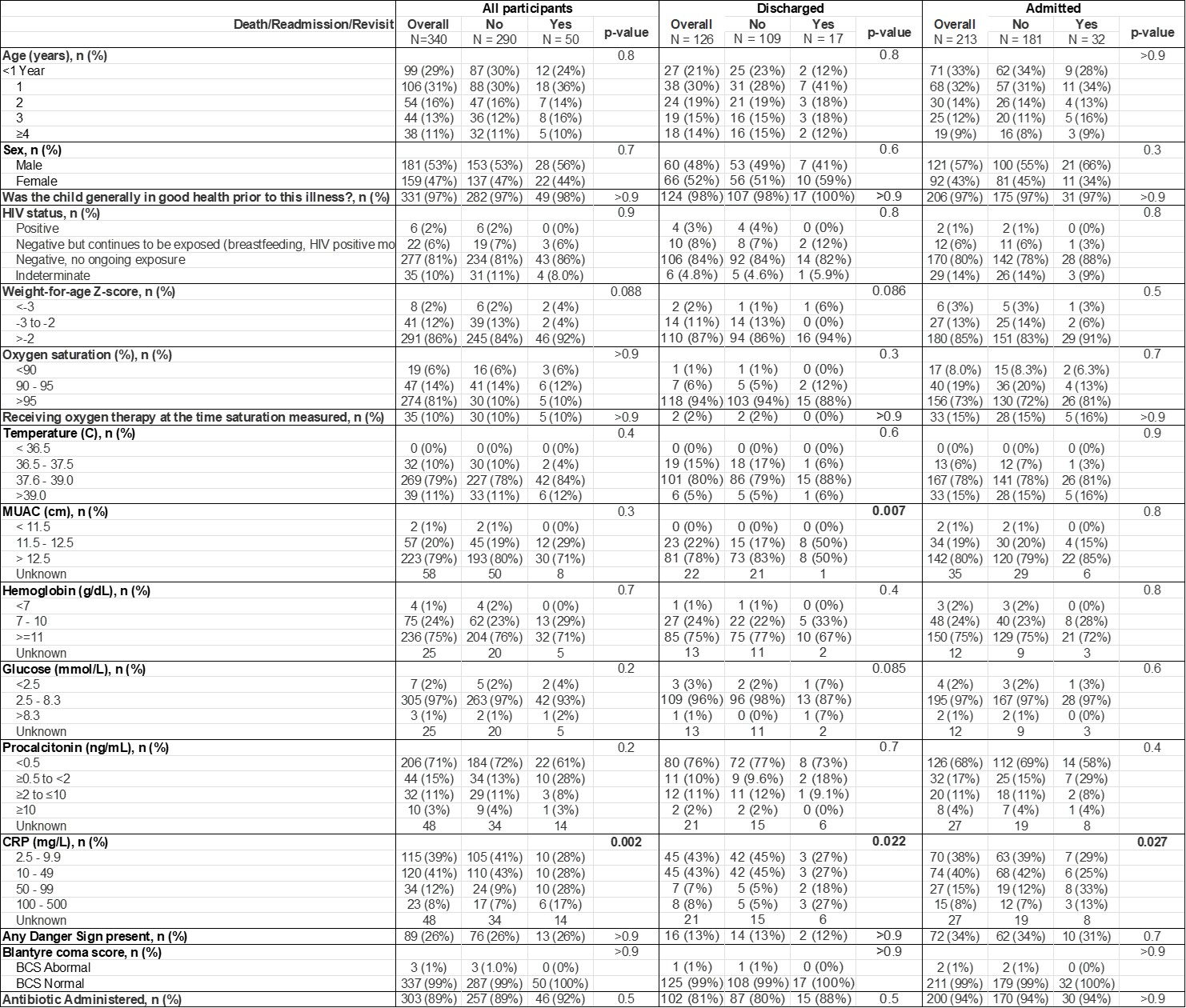 Demographic and clinical data of participants, stratified by initial disposition. Fisher’s exact test and Pearson’s Chi-squared test were utilized to determine statistical significance with a cutoff of p<0.05
Demographic and clinical data of participants, stratified by initial disposition. Fisher’s exact test and Pearson’s Chi-squared test were utilized to determine statistical significance with a cutoff of p<0.05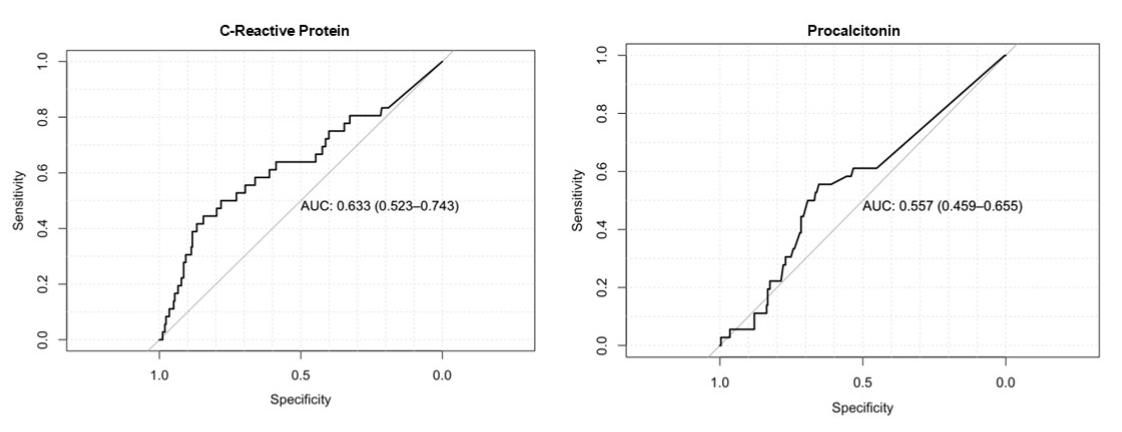 Receiver operating characteristic curves for CRP and PCT biomarkers for the primary outcome of death, readmission, or revisit
Receiver operating characteristic curves for CRP and PCT biomarkers for the primary outcome of death, readmission, or revisit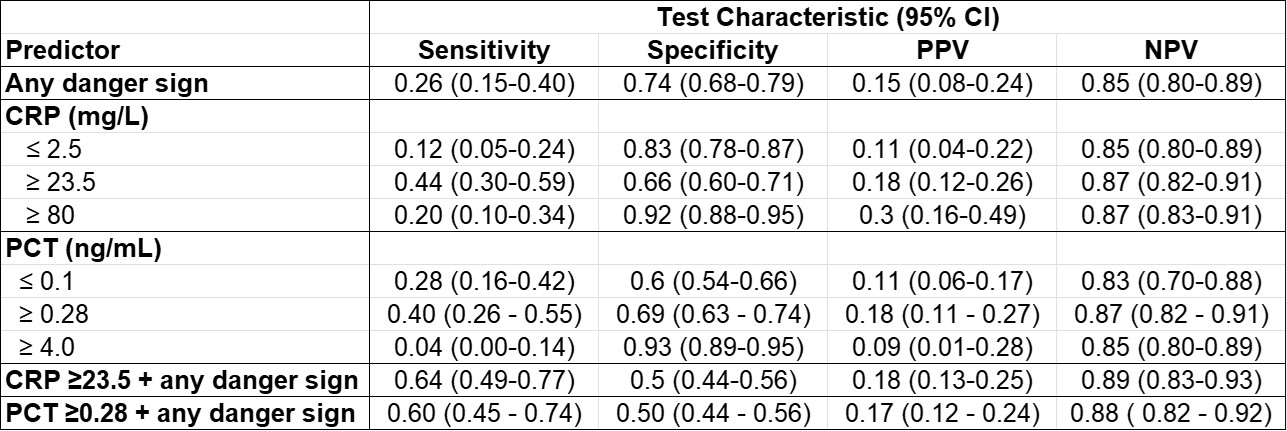 Test characteristics for any danger sign, CRP and PCT for the primary outcome of death, readmission, or revisitDemographic and clinical data of participants, stratified by initial disposition. Fisher’s exact test and Pearson’s Chi-squared test were utilized to determine statistical significance with a cutoff of p<0.05Receiver operating characteristic curves for CRP and PCT biomarkers for the primary outcome of death, readmission, or revisitTest characteristics for any danger sign, CRP and PCT for the primary outcome of death, readmission, or revisit
Test characteristics for any danger sign, CRP and PCT for the primary outcome of death, readmission, or revisitDemographic and clinical data of participants, stratified by initial disposition. Fisher’s exact test and Pearson’s Chi-squared test were utilized to determine statistical significance with a cutoff of p<0.05Receiver operating characteristic curves for CRP and PCT biomarkers for the primary outcome of death, readmission, or revisitTest characteristics for any danger sign, CRP and PCT for the primary outcome of death, readmission, or revisit