
Global Neonatal & Children's Health 2
Session: Global Neonatal & Children's Health 2

Manimaran Ramani, MD
Chief Medical Officer
University of Alabama School of Medicine
Mobile, Alabama, United States
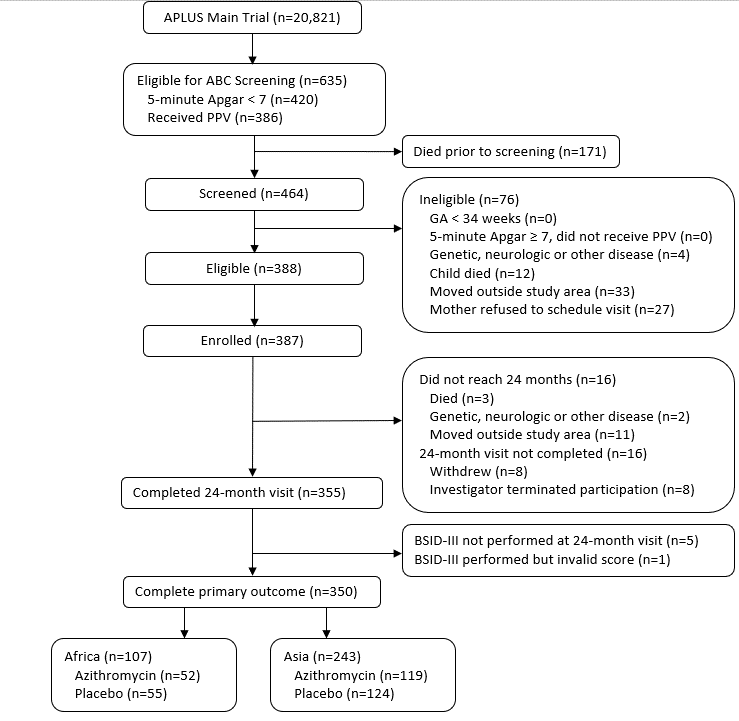 CONSORT Diagram
CONSORT Diagram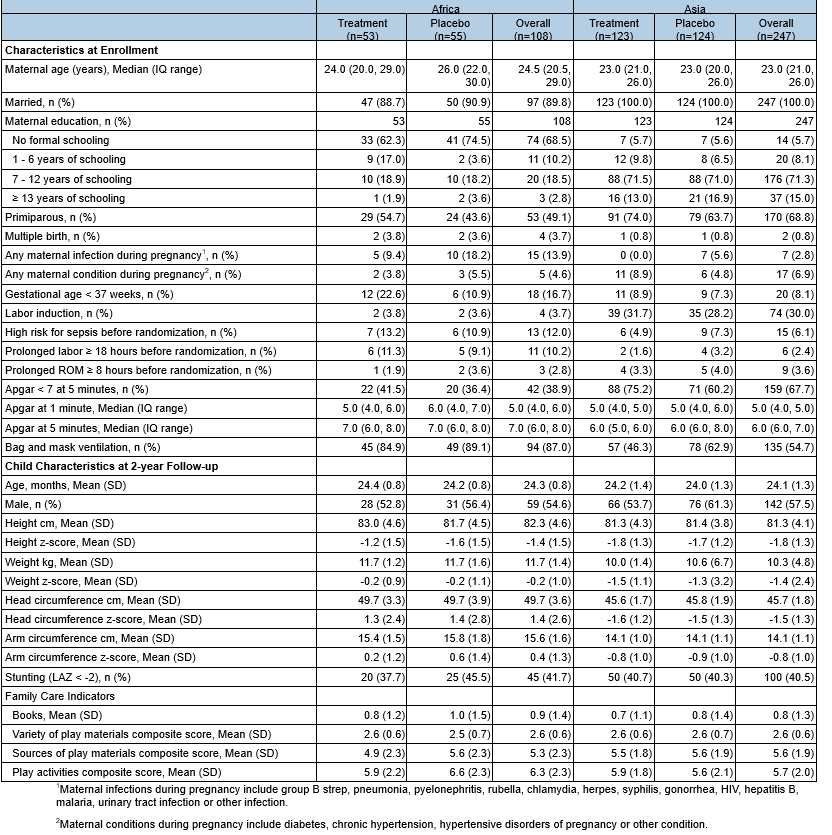 1 Maternal infections during pregnancy include group B strep, pneumonia, pyelonephritis, rubella, chlamydia, herpes, syphilis, gonorrhea, HIV, hepatitis B, malaria, urinary tract infection or other infection.
1 Maternal infections during pregnancy include group B strep, pneumonia, pyelonephritis, rubella, chlamydia, herpes, syphilis, gonorrhea, HIV, hepatitis B, malaria, urinary tract infection or other infection.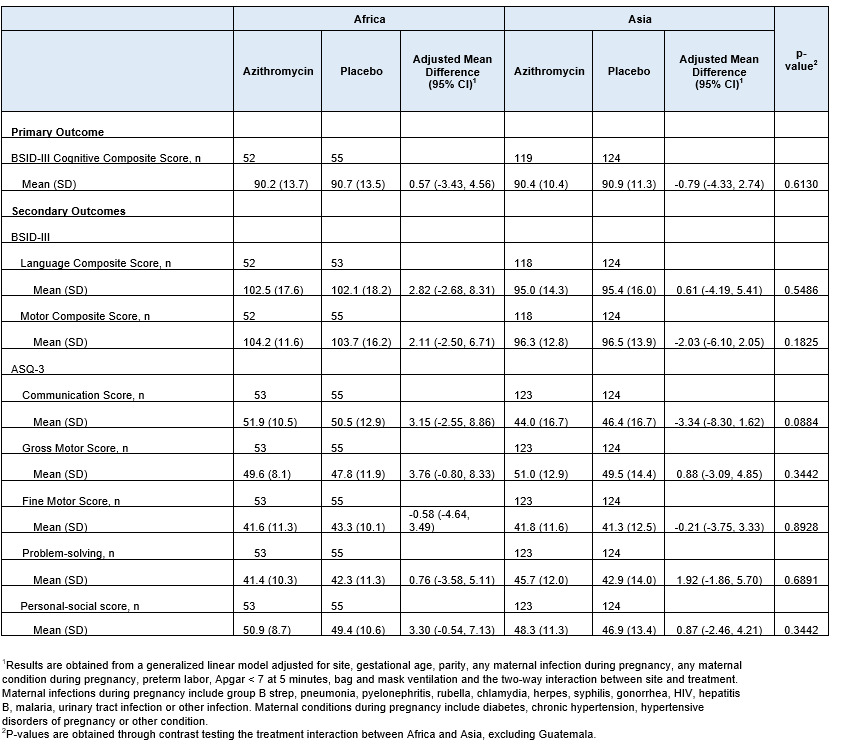 1 Results are obtained from a generalized linear model adjusted for site, gestational age, parity, any maternal infection during pregnancy, any maternal condition during pregnancy, preterm labor, Apgar < 7 at 5 minutes, bag and mask ventilation and the two-way interaction between site and treatment. Maternal infections during pregnancy include group B strep, pneumonia, pyelonephritis, rubella, chlamydia, herpes, syphilis, gonorrhea, HIV, hepatitis B, malaria, urinary tract infection or other infection. Maternal conditions during pregnancy include diabetes, chronic hypertension, hypertensive disorders of pregnancy or other condition.
1 Results are obtained from a generalized linear model adjusted for site, gestational age, parity, any maternal infection during pregnancy, any maternal condition during pregnancy, preterm labor, Apgar < 7 at 5 minutes, bag and mask ventilation and the two-way interaction between site and treatment. Maternal infections during pregnancy include group B strep, pneumonia, pyelonephritis, rubella, chlamydia, herpes, syphilis, gonorrhea, HIV, hepatitis B, malaria, urinary tract infection or other infection. Maternal conditions during pregnancy include diabetes, chronic hypertension, hypertensive disorders of pregnancy or other condition.