
Emergency Medicine 1
Session: Emergency Medicine 1
 Credit")
 photo")
Jason Metcalf, MD, PhD, FAAP (he/him/his)
Physician Lead, Pediatric Clinical Teaching Unit
Windsor Regional Hospital
Windsor, Ontario, Canada
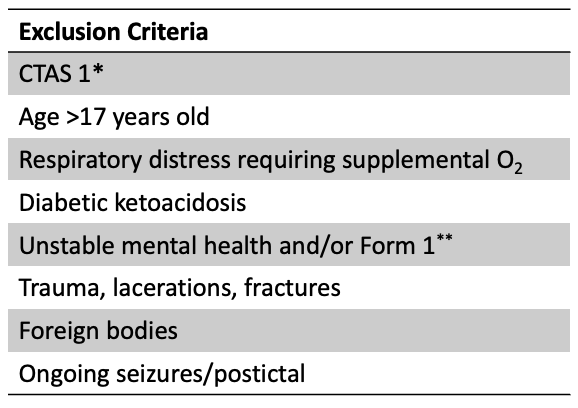 * Canadian Triage and Acuity Scale (CTAS).
* Canadian Triage and Acuity Scale (CTAS).
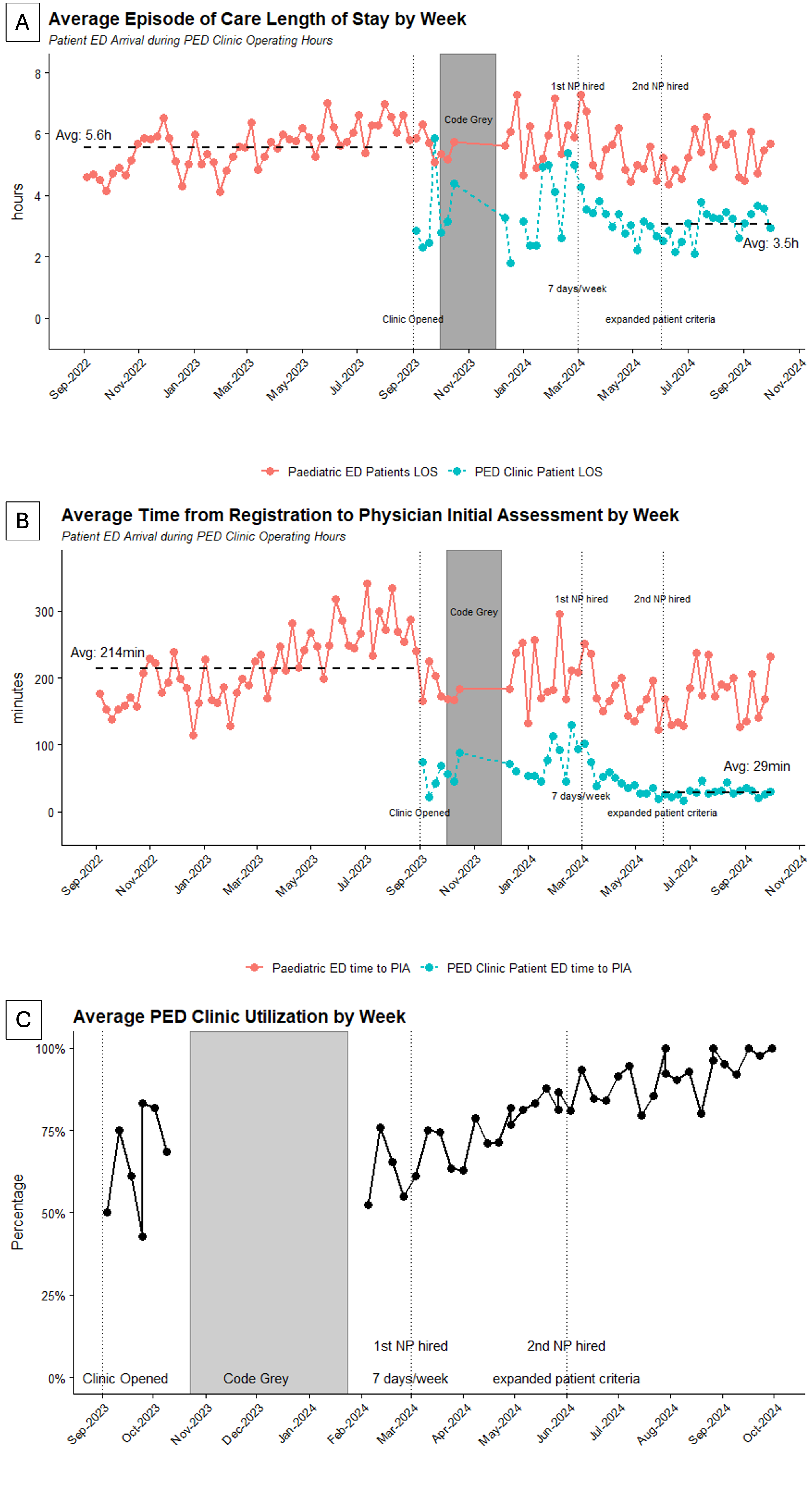 A) Average patient total length of stay by week. Code Grey indicates a period of time when hospital data systems were down and data was unable to be collected. B) Average time from registration to provider initial assessment. C) Clinic utilization rate by week, indicating the percentage of patients meeting criteria for PEDs clinic who were transferred to the clinic for assessment.
A) Average patient total length of stay by week. Code Grey indicates a period of time when hospital data systems were down and data was unable to be collected. B) Average time from registration to provider initial assessment. C) Clinic utilization rate by week, indicating the percentage of patients meeting criteria for PEDs clinic who were transferred to the clinic for assessment.