017 - Analysis of Poison Center Pediatric Health Care Facility Referral Refusals: Data from the National Poison Data System (2009-2023)
Friday, April 25, 2025
5:30pm - 7:45pm HST
Publication Number: 17.3897
Anna Zmuda, University of Virginia School of Medicine, Charlottesville, VA, United States; Sage Timberline, University of Virginia, Charlottesville, VA, United States; Rita Farah, University of Virginia School of Medicine, CHARLOTTESVILLE, VA, United States; Jennifer R Charlton, University of Virginia School of Medicine, charlottesville, VA, United States; Nathan P. Charlton, University of Virginia School of Medicine, Charlottesville, VA, United States
Fellow University of Virginia Charlottesville, Virginia, United States
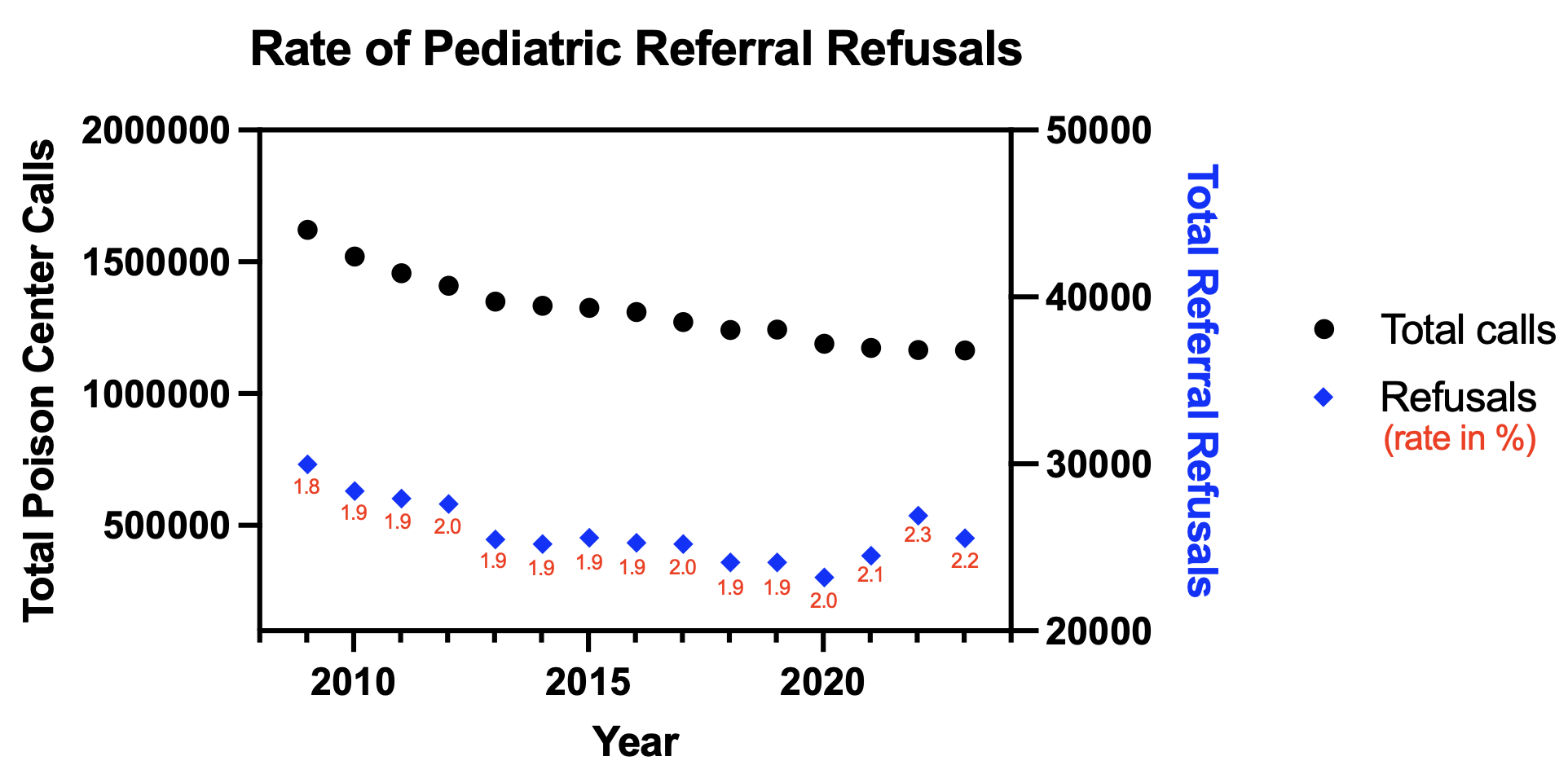
Background: Approximately 1.1 million cases of xenobiotic exposures in persons ≤19 are called to United States (US) Poison Centers (PC) each year, representing roughly half of all PC cases. The majority of cases are unintentional exposures and 78% of these cases are managed at home, with 22% referred to the hospital for evaluation. Less than 2% of all PC callers refuse referral to a health care facility (HCF) when advised to do so by the PC, but less is known about the pediatric population. Objective: This study aimed to identify number of yearly pediatric HCF referral refusals and to characterize the xenobiotics most often associated. Design/Methods: This was a retrospective study of pediatric reports to the US National Poison Data System over a 15-year period from January 1st, 2009 to December 31st 2023. The NPDS was queried for single-substance exposures via all exposure routes in patients ≤19 years old. We assessed total number of patients, age and the xenobiotics involved. Results: Over the study period there were 152,485 calls (average 10,165 yearly) in which callers refused referral to a HCF. The peak number of refusals was 14,954 in 2009, with a low of 7,895 in 2023. However, total yearly PC calls declined over the study period, so the rate of refusal remained fairly consistent, ranging from 1.8-2.3% with an average of 2.0% overall. Referral was refused most commonly for teenagers (13-19), with an average of 3305 (32%) refusals yearly, followed by age 2 (n=1904, 19%) and age 1 (n=1650, 16%). Acetaminophen products (418 cases yearly, 4%) were the single substance most often associated with refusal, followed by ibuprofen (n=377, 4%) and miscellaneous unknown drugs (n=344, 3%). The main cause of exposure was unintentional (n=104,913, 45%), followed by suspected suicide (n=22,290, 15%). Vomiting was the symptom most often associated with refusal (10% of cases) and drowsiness/lethargy comprised 6% of cases.
Conclusion(s): While total number of pediatric refusals to HCFs declined over the 15-year period, the rate remained relatively stable. Unintentional exposures to relatively innocuous medications may not require further follow up by PC staff. However, suspected suicide, comprising 15% of cases, and cases involving dangerous xenobiotics such as acetaminophen, comprising 4% of cases, require more PC and first responder services, such as welfare checks. There were a large variety of agents involved, with no single agent making up than 4% of the total. Additional work is needed to determine the reasons for refusal to HCFs, outcomes and whether PC training interventions would decrease the rate of refusal.