
Neonatal Pulmonology - Basic/Translational Science 2
Session: Neonatal Pulmonology - Basic/Translational Science 2
 photo")
Samuel Gentle, MD (he/him/his)
Assistant Professor
Yale School of Medicine
New Haven, Connecticut, United States
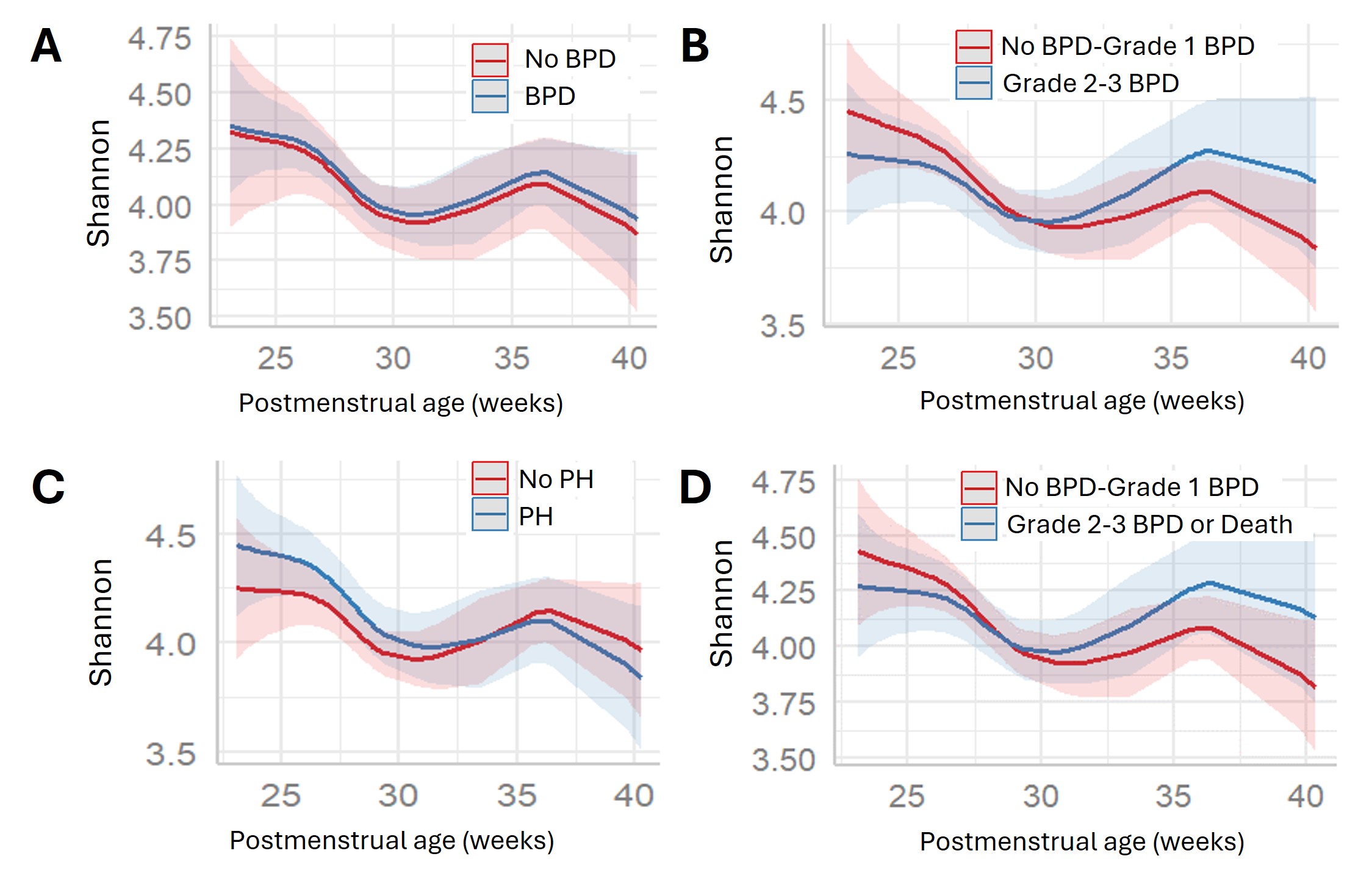 Alpha diversity plots over time between comparison groups of A: No BPD vs BPD, B: No BPD/Grade 1 BPD vs Grade 2-3 BPD, C: No pulmonary hypertension vs Pulmonary Hypertension, and D: No BPD/Grade 1 BPD vs Grade 2-3 BPD or death. No measures of alpha diversity significantly differed by comparison groups (A: p=0.96, B: p=0.07, C: p=0.22, D: p=0.09).
Alpha diversity plots over time between comparison groups of A: No BPD vs BPD, B: No BPD/Grade 1 BPD vs Grade 2-3 BPD, C: No pulmonary hypertension vs Pulmonary Hypertension, and D: No BPD/Grade 1 BPD vs Grade 2-3 BPD or death. No measures of alpha diversity significantly differed by comparison groups (A: p=0.96, B: p=0.07, C: p=0.22, D: p=0.09).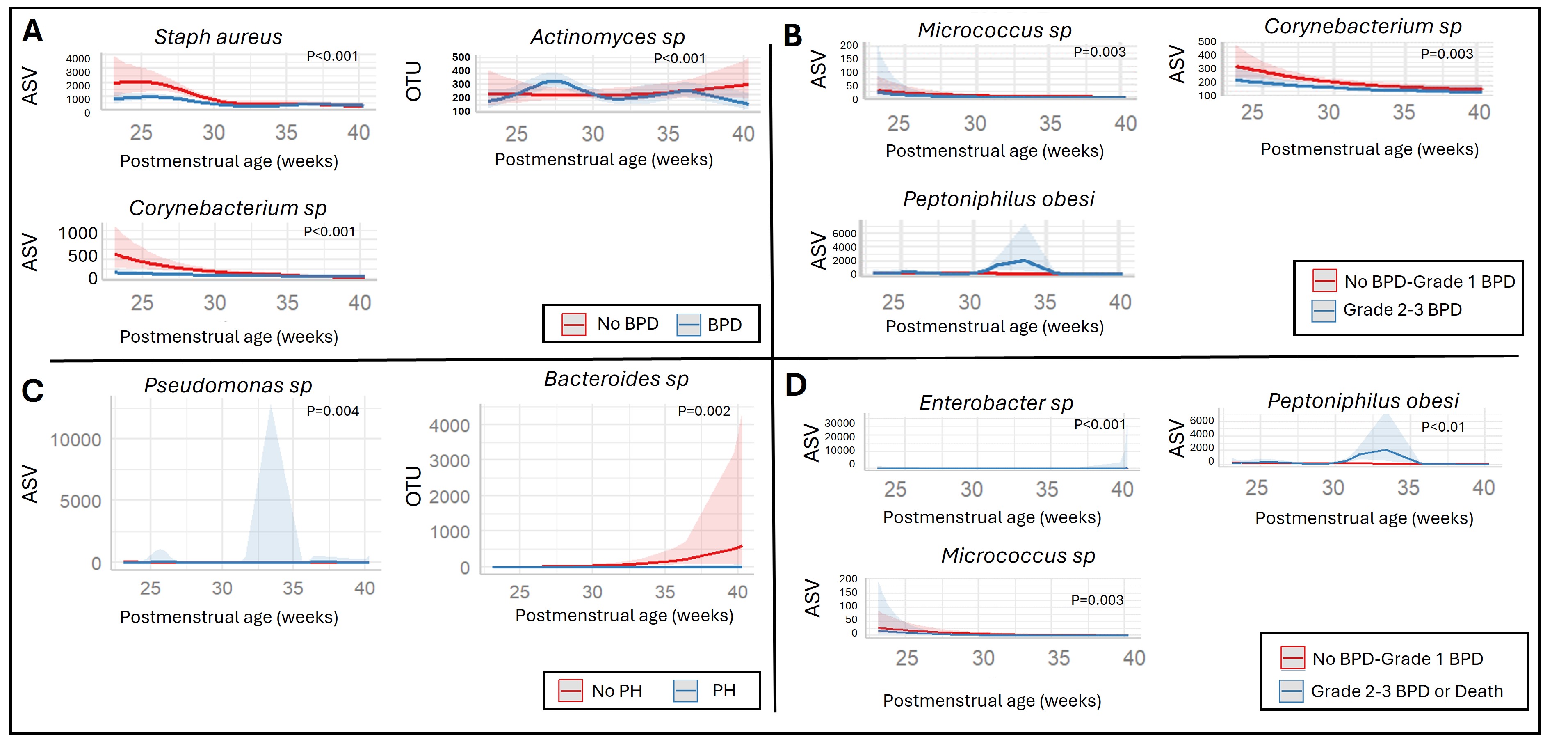 Single-taxon significant differences over time between comparison groups of A: No BPD vs BPD, B: No BPD/Grade 1 BPD vs Grade 2-3 BPD, C: No pulmonary hypertension vs Pulmonary Hypertension, and D: No BPD/Grade 1 BPD vs Grade 2-3 BPD or death.
Single-taxon significant differences over time between comparison groups of A: No BPD vs BPD, B: No BPD/Grade 1 BPD vs Grade 2-3 BPD, C: No pulmonary hypertension vs Pulmonary Hypertension, and D: No BPD/Grade 1 BPD vs Grade 2-3 BPD or death. 