
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
Stephanie Yeager, MD (she/her/hers)
Neonatal-Perinatal Fellow
Seattle Children's/University of Washington
Seattle, Washington, United States
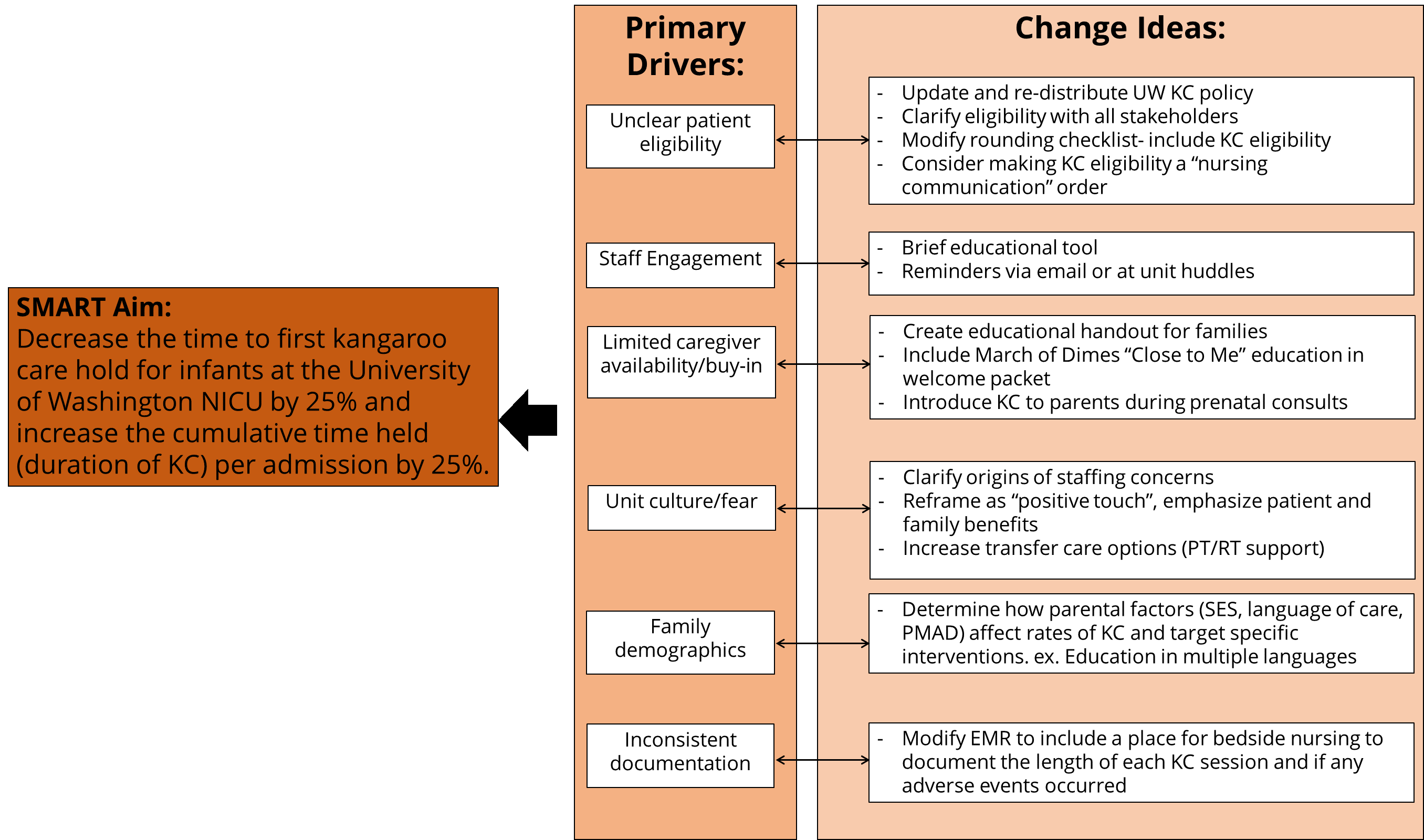 Driver Diagram for Improving Rates of Kangaroo Care in the University of Washington NICU
Driver Diagram for Improving Rates of Kangaroo Care in the University of Washington NICU.png) Demographics and Balancing Measures
Demographics and Balancing Measures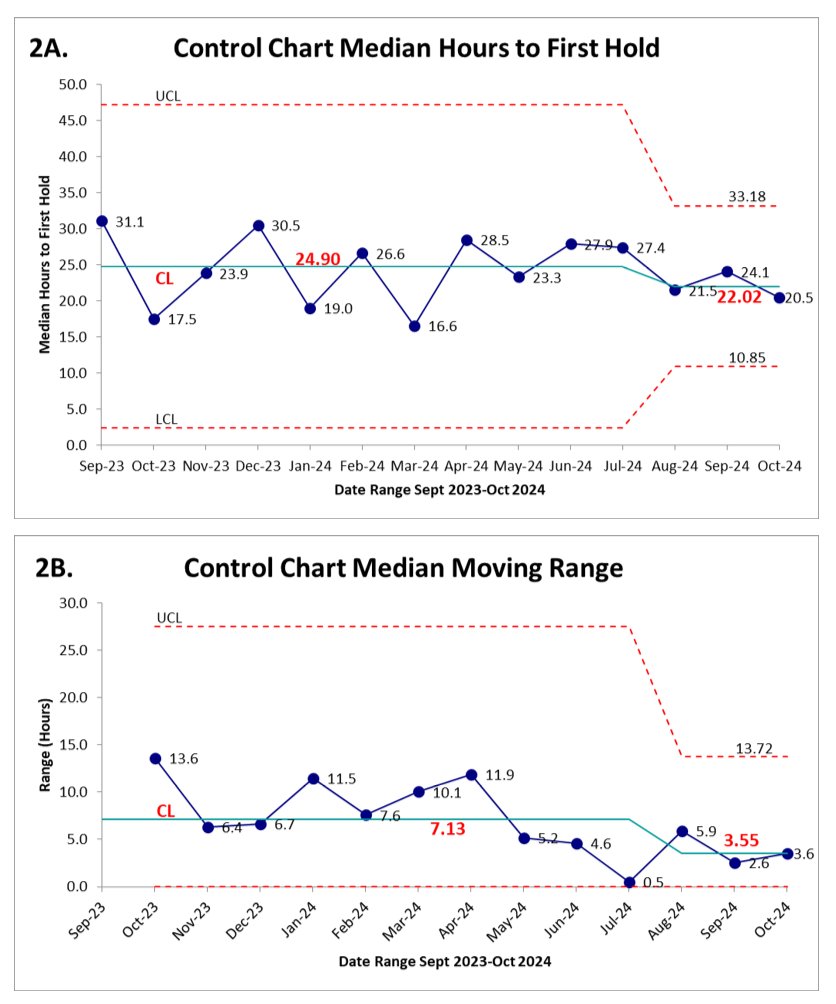 No sustained change in hours to first kangaroo care hold post PDSA #1 (January 2024) or PDSA #2 (March 2024), early signs of improvement and process standardization after PDSA #3 (August 2024) including narrowing of median moving range
No sustained change in hours to first kangaroo care hold post PDSA #1 (January 2024) or PDSA #2 (March 2024), early signs of improvement and process standardization after PDSA #3 (August 2024) including narrowing of median moving range