
Cardiology 1
Session: Cardiology 1

Christiane Mhanna, D.O.
Pediatric Cardiology Fellow
Nemours Children's Hospital
Wilmington, Delaware, United States
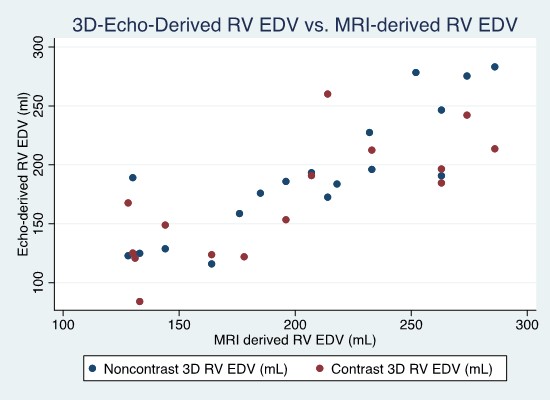 Scatter plot of noncontrast and contrast 3DE derived RVEDV versus CMR derived RVEDV.
Scatter plot of noncontrast and contrast 3DE derived RVEDV versus CMR derived RVEDV. 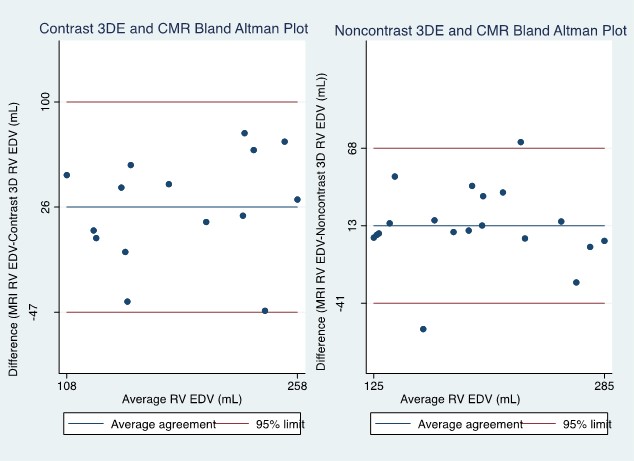 Bland Altman Plot of contrast 3DE, noncontrast 3DE and CMR derived RVEDV.
Bland Altman Plot of contrast 3DE, noncontrast 3DE and CMR derived RVEDV. 