
Neonatal Hemodynamics and Cardiovascular Medicine 1
Session: Neonatal Hemodynamics and Cardiovascular Medicine 1
Priya R. Gupta, BA, BS (she/her/hers)
Medical Student
University of Connecticut School of Medicine
Farmington, Connecticut, United States
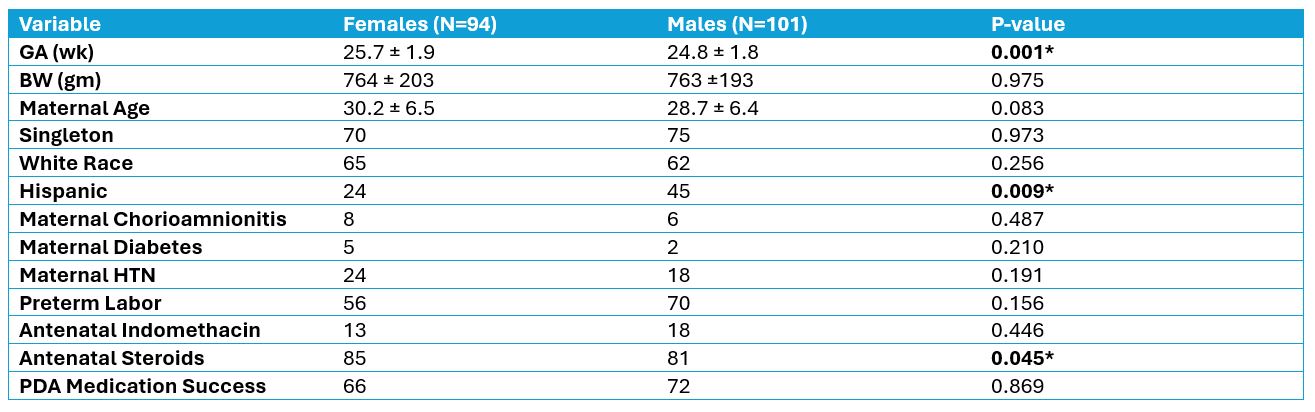 Statistical analysis using Chi-square tests and Student’s T-tests.
Statistical analysis using Chi-square tests and Student’s T-tests. 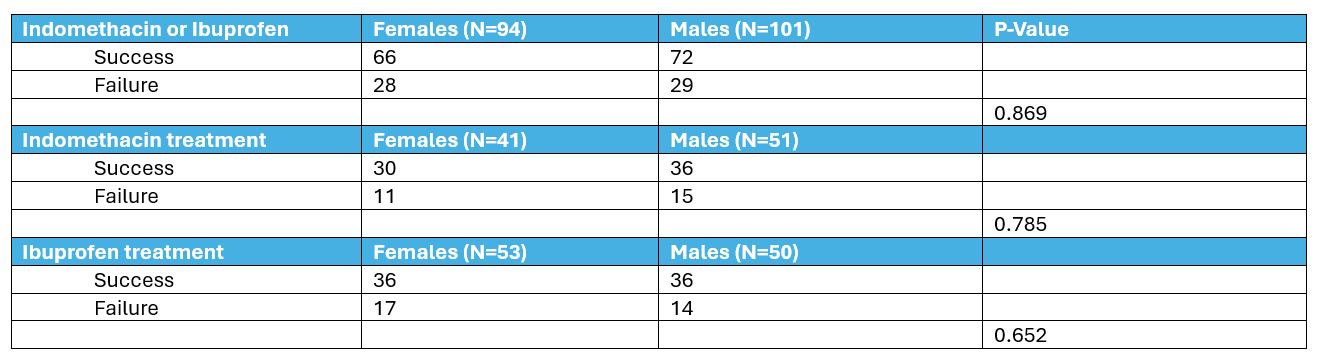 Failure of initial medical treatment was defined as the need for subsequent medical retreatment or surgical / catheter closure of PDA.
Failure of initial medical treatment was defined as the need for subsequent medical retreatment or surgical / catheter closure of PDA.