
Neonatal Hemodynamics and Cardiovascular Medicine 1
Session: Neonatal Hemodynamics and Cardiovascular Medicine 1
 photo")
Tamorah R. Lewis, MD, PhD (she/her/hers)
Associate Professor
The Hospital for Sick Children
Toronto, Ontario, Canada
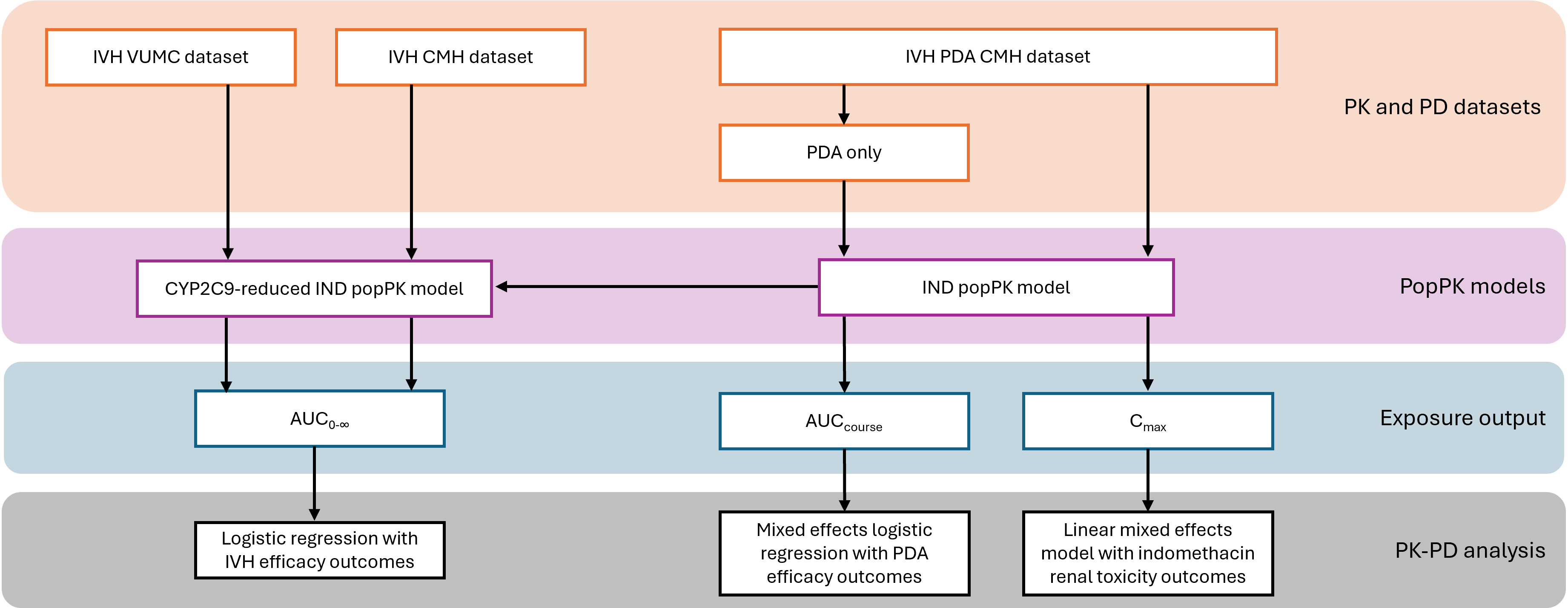 The descriptions of the main steps are presented on the right within their color-coded boxes from orange to grey. The vertical arrows represent steps for producing patient-specific PK parameters and subsequent PK-PD analyses. The horizontal arrow represents the model modification of the published IND popPK model to develop a CYP2C9-reduced IND popPK model. IVH: intraventricular hemorrhage; PDA: patent ductus arteriosus; VUMC: Vanderbilt University Medical Center; CMH: Children’s Mercy Hospital; AUC: area under the curve; IND: indomethacin; popPK: population pharmacokinetics; PK: pharmacokinetics; PD: pharmacodynamics.
The descriptions of the main steps are presented on the right within their color-coded boxes from orange to grey. The vertical arrows represent steps for producing patient-specific PK parameters and subsequent PK-PD analyses. The horizontal arrow represents the model modification of the published IND popPK model to develop a CYP2C9-reduced IND popPK model. IVH: intraventricular hemorrhage; PDA: patent ductus arteriosus; VUMC: Vanderbilt University Medical Center; CMH: Children’s Mercy Hospital; AUC: area under the curve; IND: indomethacin; popPK: population pharmacokinetics; PK: pharmacokinetics; PD: pharmacodynamics. 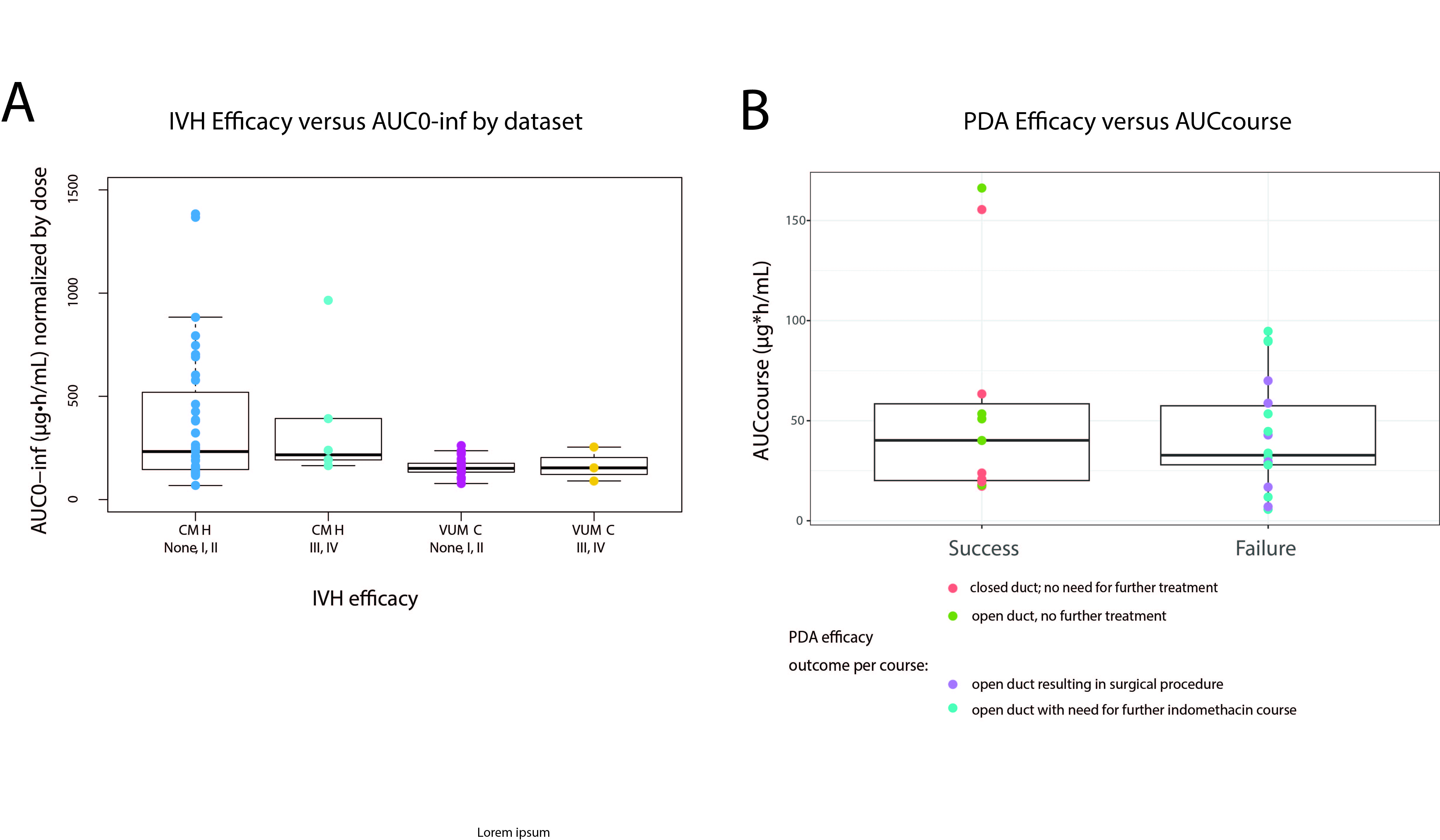 A) AUC0-∞ across intraventricular hemorrhage (IVH) efficacy outcome by severity: non-severe (none, grade I, grade II) and severe (grade III, grade IV), shown per study site (CMH: Children’s Mercy Hospital and VUMC: Vanderbilt University Medical Center). B) AUCcourse across patent ductus arteriosus (PDA) efficacy outcome by severity: success (no further treatment needed) and failure (further indomethacin dose or surgical procedure needed).
A) AUC0-∞ across intraventricular hemorrhage (IVH) efficacy outcome by severity: non-severe (none, grade I, grade II) and severe (grade III, grade IV), shown per study site (CMH: Children’s Mercy Hospital and VUMC: Vanderbilt University Medical Center). B) AUCcourse across patent ductus arteriosus (PDA) efficacy outcome by severity: success (no further treatment needed) and failure (further indomethacin dose or surgical procedure needed).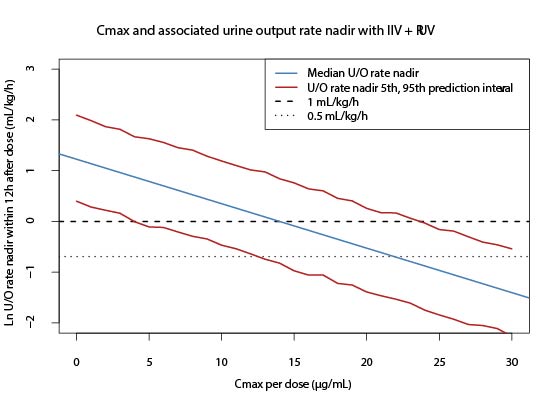 Cmax and associated ln of U/O rate nadir within 12 hours after dose with simulated median, and 5th and 95th prediction interval U/O rate nadir within 12 hours after dose. Both interindividual variability (IIV) and residual unexplained variability (RUV) were used in the simulation. Extrapolation of data was extended past U/O rate nadir within 12 hours after dose <0.5 mL/kg/h and <1 mL/kg/h.
Cmax and associated ln of U/O rate nadir within 12 hours after dose with simulated median, and 5th and 95th prediction interval U/O rate nadir within 12 hours after dose. Both interindividual variability (IIV) and residual unexplained variability (RUV) were used in the simulation. Extrapolation of data was extended past U/O rate nadir within 12 hours after dose <0.5 mL/kg/h and <1 mL/kg/h.