
Emergency Medicine 1
Session: Emergency Medicine 1
Kayle Randolph, DO (she/her/hers)
Pediatric Emergency Medicine Fellow
Children's Mercy Hospitals and Clinics
Mission, Kansas, United States
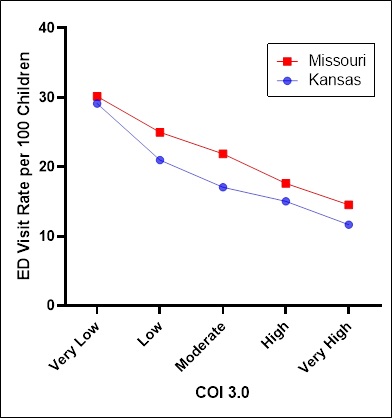 Lower Childhood Opportunity Index (COI) was associated with higher Emergency Department (ED) Utilization
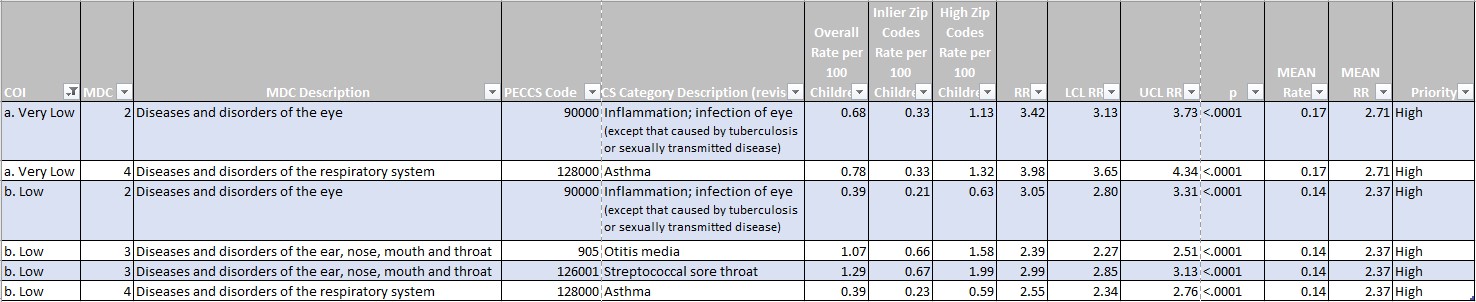
Lower Childhood Opportunity Index (COI) was associated with higher Emergency Department (ED) Utilization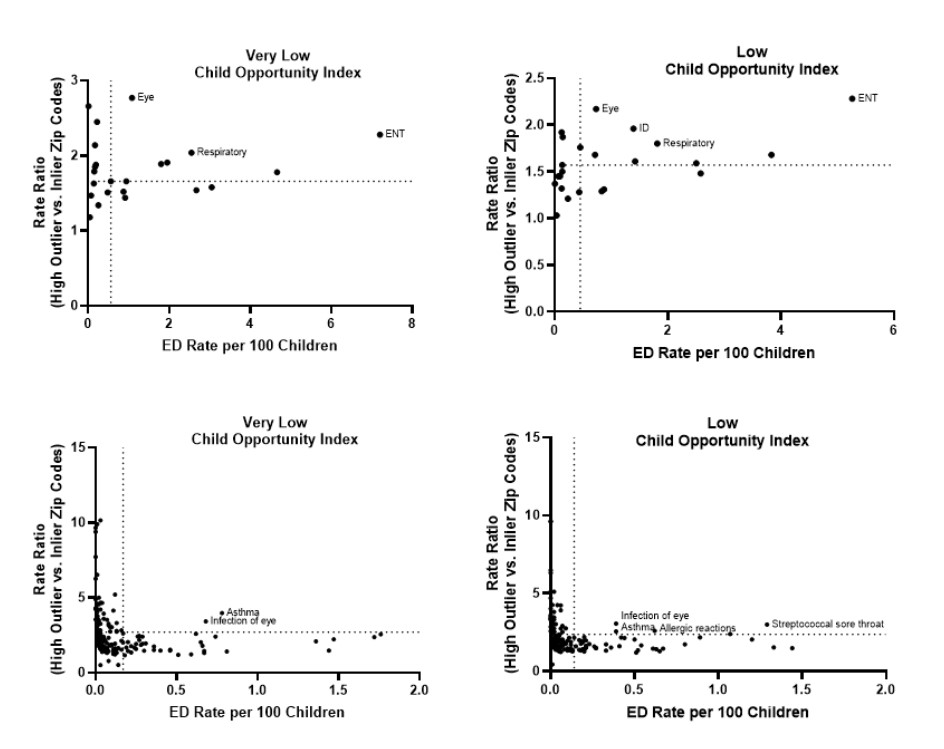 Upper two graphs depict highest outlying diagnoses by Major Diagnostic Criteria (MDC), from Very Low and Low COI groups.
Upper two graphs depict highest outlying diagnoses by Major Diagnostic Criteria (MDC), from Very Low and Low COI groups.