
Quality Improvement/Patient Safety 2
Session: Quality Improvement/Patient Safety 2
 Credit")
 photo")
Sabrina E. Carro, MD (she/her/hers)
Fellow
Monroe Carell Jr. Children's Hospital at Vanderbilt
Nashville, Tennessee, United States
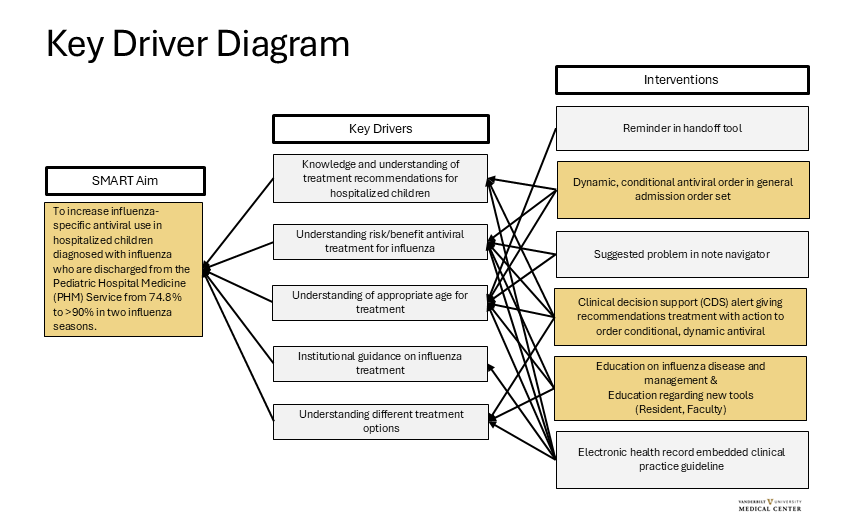 A Key Driver Diagram was created with a multi-disciplinary team including: pediatric hospital medicine, pediatric infectious diseases, pharmacy, and clinical informatics. Children are diagnosed with influenza by respiratory testing either at our institution or at an outside institution within 5 days of admission. Interventions in gold shaded boxes are in progress. The dynamic, conditional orders uses logic to display an oseltamivir order with the appropriate age and weight-based dose during the admission workflow. If respiratory testing comes back after that workflow, a delayed alert will display prompting the clinician to order an antiviral. There is logic to suppress the alert if an antiviral is ordered or if one dose has been successfully administered. In the alert, the clinician is encouraged to discuss this recommendation with family if not already addressed. Additionally, the alert can be dismissed for the rest of the encounter if the family prefers to not treat with an antiviral. Interventions in grey shaded boxes are potential future interventions.
A Key Driver Diagram was created with a multi-disciplinary team including: pediatric hospital medicine, pediatric infectious diseases, pharmacy, and clinical informatics. Children are diagnosed with influenza by respiratory testing either at our institution or at an outside institution within 5 days of admission. Interventions in gold shaded boxes are in progress. The dynamic, conditional orders uses logic to display an oseltamivir order with the appropriate age and weight-based dose during the admission workflow. If respiratory testing comes back after that workflow, a delayed alert will display prompting the clinician to order an antiviral. There is logic to suppress the alert if an antiviral is ordered or if one dose has been successfully administered. In the alert, the clinician is encouraged to discuss this recommendation with family if not already addressed. Additionally, the alert can be dismissed for the rest of the encounter if the family prefers to not treat with an antiviral. Interventions in grey shaded boxes are potential future interventions. .png) P-Chart of hospital admission encounters of children diagnosed with influenza who were discharged from the Pediatric Hospital Medicine (PHM) service that had at least one successful administration of an influenza-specific antiviral. The first intervention was a hospital-wide Grand Rounds. Other educational interventions were targeted to either PHM faculty or residents. For the dynamic order and CDS alert interventions, there was resident education on the new tool as part of standard change management best practices. Baseline: 74.8%, Goal Line: 90%. Abbreviation: CDS: Clinical Decision Support.
P-Chart of hospital admission encounters of children diagnosed with influenza who were discharged from the Pediatric Hospital Medicine (PHM) service that had at least one successful administration of an influenza-specific antiviral. The first intervention was a hospital-wide Grand Rounds. Other educational interventions were targeted to either PHM faculty or residents. For the dynamic order and CDS alert interventions, there was resident education on the new tool as part of standard change management best practices. Baseline: 74.8%, Goal Line: 90%. Abbreviation: CDS: Clinical Decision Support..png) X-bar chart with average time to an antiviral medication order signed by a clinician. If a respiratory test was obtained during the encounter, the time from the test result to order signed was used. If the test was prior to the current encounter, the time from presentation to the emergency department to order signed was used. There was special cause variation with 8 points below the mean causing a shift in the center line from 4.9 hours to 2.4 hours after educational interventions. There was also special cause variation with one point outside the upper control limit at points (1), (2), and (3). Each implicated encounter underwent manual chart review. In (1), there was a delay in an antiviral medication order signed in two of the three encounters for that data point. The first was due to escalating respiratory support with inability to obtain enteral access via a nasogastric tube and the second was due to the patient having repeated emesis resulting in an order delay and successful administration. At (2), the family preferred to discuss further before proceeding with treatment which led to the delay. At (3), there was a miscommunication during care handoffs as to whether the patient completed an oseltamivir treatment course outpatient prior to admission.
X-bar chart with average time to an antiviral medication order signed by a clinician. If a respiratory test was obtained during the encounter, the time from the test result to order signed was used. If the test was prior to the current encounter, the time from presentation to the emergency department to order signed was used. There was special cause variation with 8 points below the mean causing a shift in the center line from 4.9 hours to 2.4 hours after educational interventions. There was also special cause variation with one point outside the upper control limit at points (1), (2), and (3). Each implicated encounter underwent manual chart review. In (1), there was a delay in an antiviral medication order signed in two of the three encounters for that data point. The first was due to escalating respiratory support with inability to obtain enteral access via a nasogastric tube and the second was due to the patient having repeated emesis resulting in an order delay and successful administration. At (2), the family preferred to discuss further before proceeding with treatment which led to the delay. At (3), there was a miscommunication during care handoffs as to whether the patient completed an oseltamivir treatment course outpatient prior to admission.