
Quality Improvement/Patient Safety 1
Session: Quality Improvement/Patient Safety 1
 Credit")
Laura G. Amar-Dolan, MD (she/her/hers)
Assistant Professor of Pediatrics
Tufts University School of Medicine
South Portland, Maine, United States
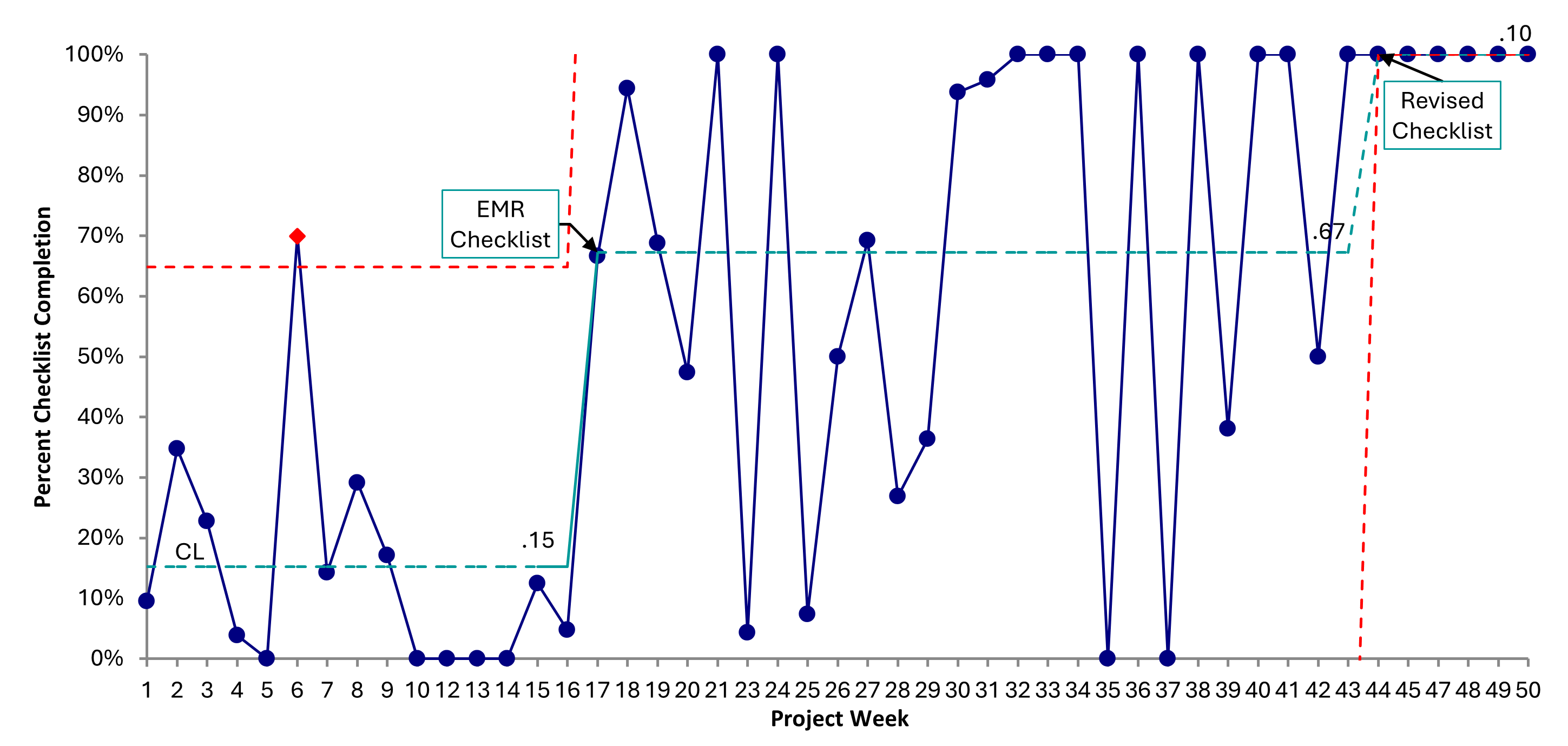 P-chart showing rates of rounding checklist completion by project week. Process changes are annotated.
P-chart showing rates of rounding checklist completion by project week. Process changes are annotated. 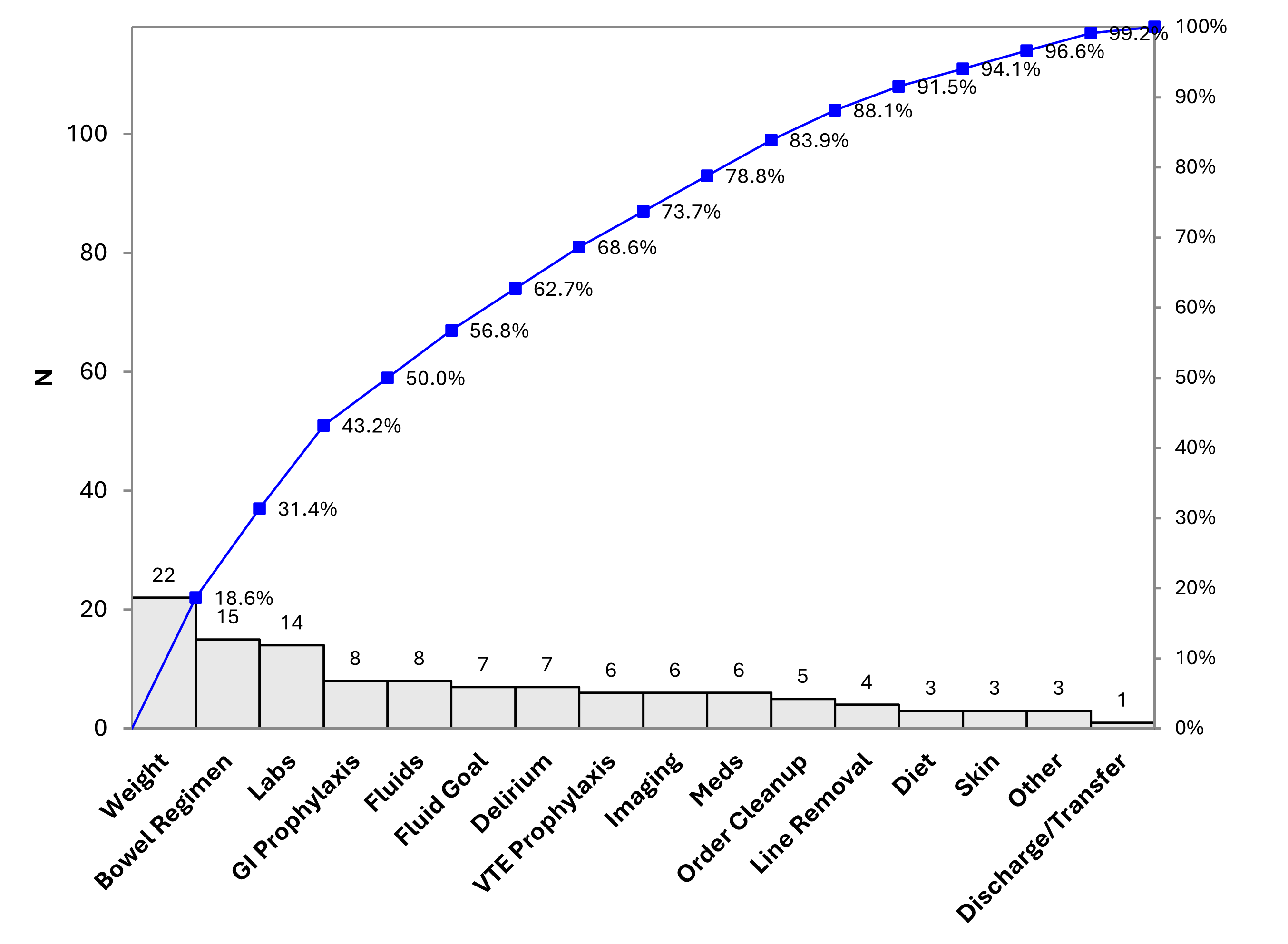 Pareto chart of care plan changes made during review of rounding checklist. P-chart showing rates of rounding checklist completion by project week. Process changes are annotated. Pareto chart of care plan changes made during review of rounding checklist.
Pareto chart of care plan changes made during review of rounding checklist. P-chart showing rates of rounding checklist completion by project week. Process changes are annotated. Pareto chart of care plan changes made during review of rounding checklist. 