
Emergency Medicine 3
Session: Emergency Medicine 3

Jamie Holland, MD
Pediatric Emergency Medicine Fellow
Northwestern University The Feinberg School of Medicine
Chicago, Illinois, United States
.png) Receiver operator curve of temperature with outcomes of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI.
Receiver operator curve of temperature with outcomes of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI.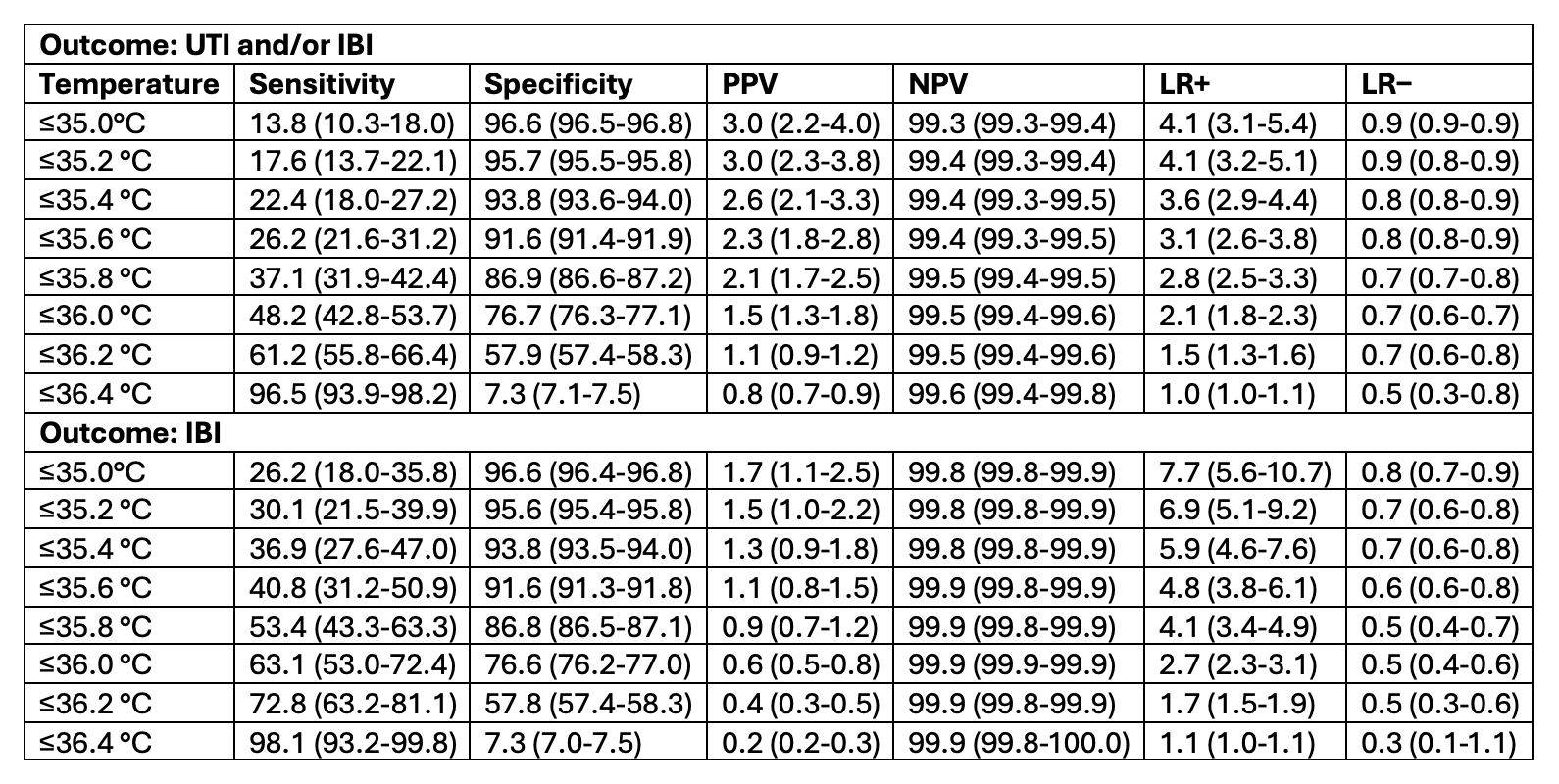 Diagnostic performance of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI identification in 0.2°C increments. Numbers in parenthesis indicate 95% confidence intervals.Receiver operator curve of temperature with outcomes of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI.Diagnostic performance of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI identification in 0.2°C increments. Numbers in parenthesis indicate 95% confidence intervals.
Diagnostic performance of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI identification in 0.2°C increments. Numbers in parenthesis indicate 95% confidence intervals.Receiver operator curve of temperature with outcomes of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI.Diagnostic performance of invasive bacterial infection (IBI) and/or urinary tract infection (UTI) and IBI identification in 0.2°C increments. Numbers in parenthesis indicate 95% confidence intervals.