
Cardiology 2
Session: Cardiology 2

Alexander P. Bruno, BS
Medical Student
Vanderbilt University School of Medicine
Nashville, Tennessee, United States
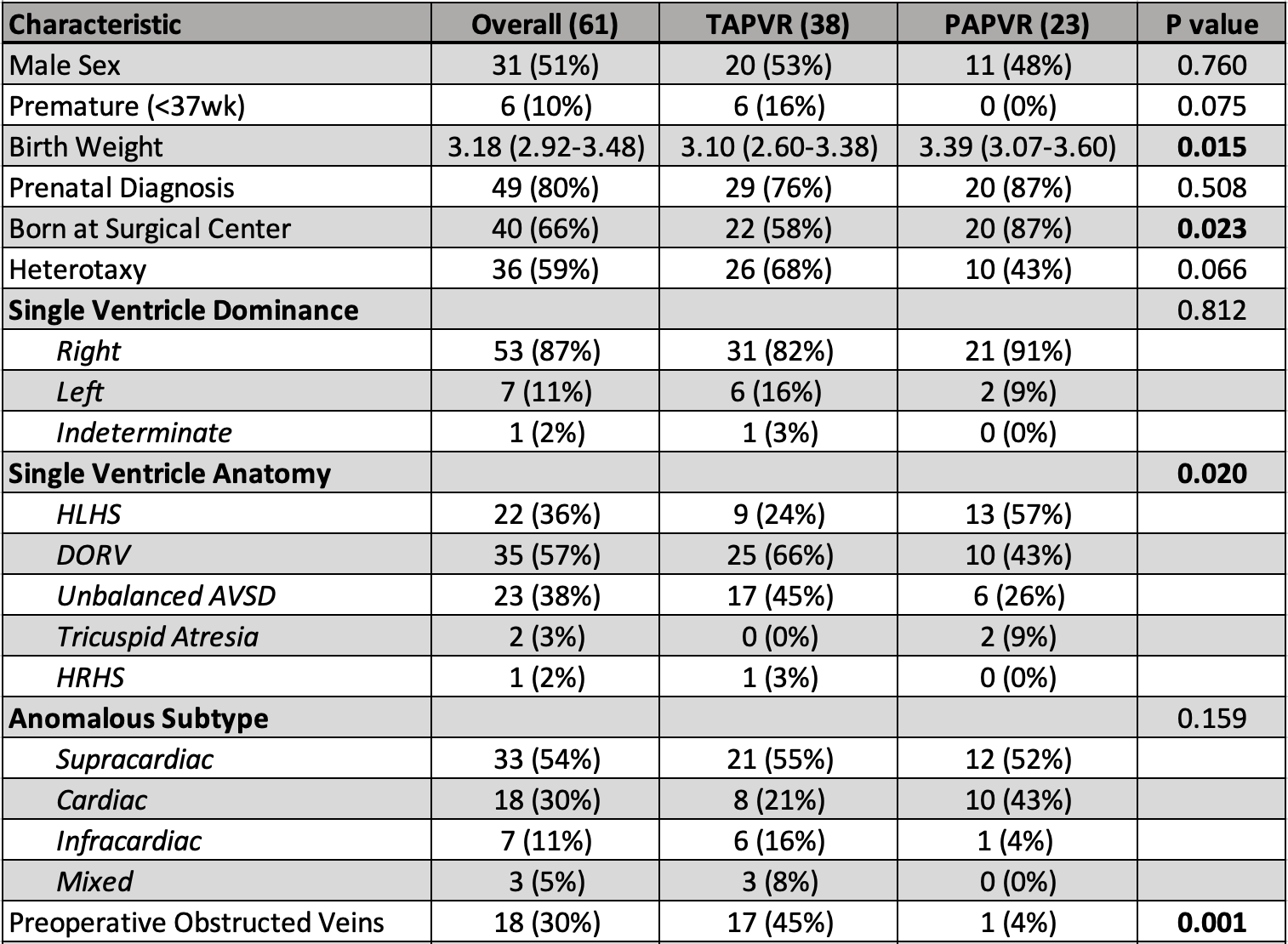 Values are median (IQR) or n (%). P-value from two-sample t-test for continuous variables or Fisher exact test for categorical variables.
Values are median (IQR) or n (%). P-value from two-sample t-test for continuous variables or Fisher exact test for categorical variables. Values are median (IQR) or n (%). P-value from two-sample t-test for continuous variables or Fisher exact test for categorical variables.
Values are median (IQR) or n (%). P-value from two-sample t-test for continuous variables or Fisher exact test for categorical variables.