
Quality Improvement/Patient Safety 1
Session: Quality Improvement/Patient Safety 1
 Credit")
 photo")
Diana Carolina Largo Luna, MD (she/her/hers)
Pediatric Resident
The Unterberg Children's Hospital at Monmouth Medical Center
Long Branch, New Jersey, United States
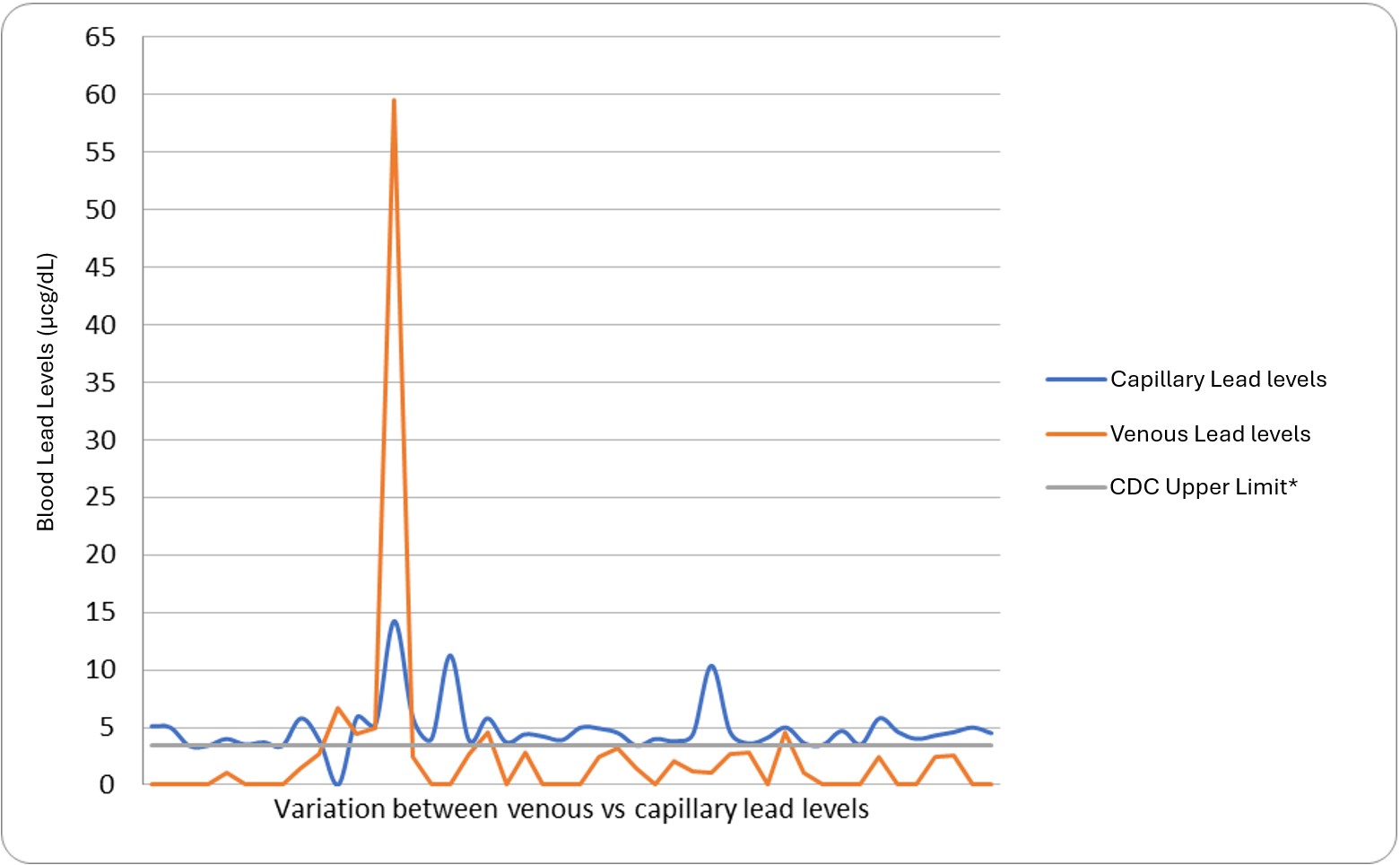 CDC (Center for Disease Control and Prevention), *CDC Upper Limit: 3.5 micrograms per deciliter.CDC (Center for Disease Control and Prevention), *CDC Upper Limit: 3.5 micrograms per deciliter.
CDC (Center for Disease Control and Prevention), *CDC Upper Limit: 3.5 micrograms per deciliter.CDC (Center for Disease Control and Prevention), *CDC Upper Limit: 3.5 micrograms per deciliter.