
Genomics/Epigenomics 1
Session: Genomics/Epigenomics 1
 photo")
Alexandra C. Keefe, MD, PHD (she/her/hers)
Assistant Professor
Seattle Children's Hospital / University of Washington
Seattle, Washington, United States
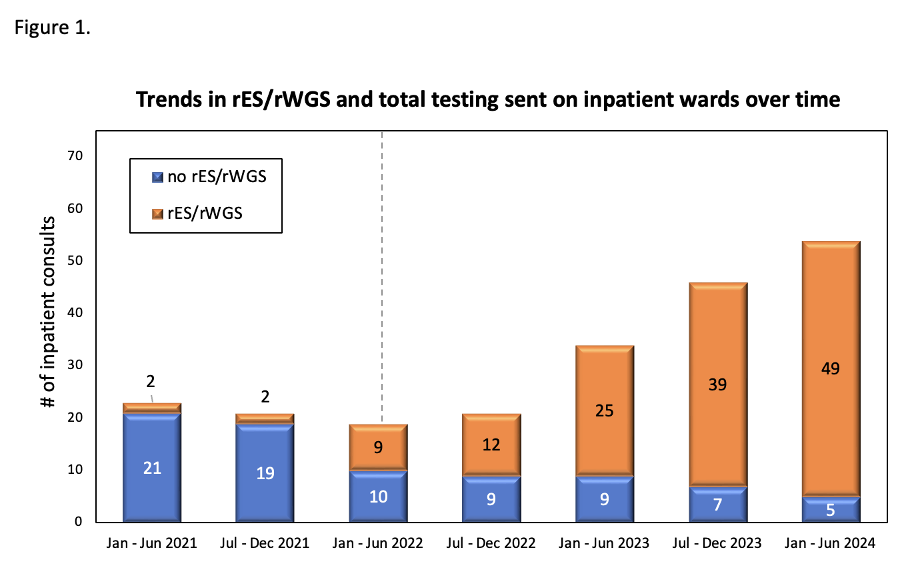 Clinical ordering patterns for genetics consults from January 2021-June 2024 as assessed in 6 month intervals. Over the study period there was a steady increase in the number of consults requested and also in the percentage of consults in which rES/rWGS was recommended and ordered by the inpatient genetics consultation service. Dashed line denotes date policy change on May 4, 2022 allowing first tier rES/rWGS for inpatients.
Clinical ordering patterns for genetics consults from January 2021-June 2024 as assessed in 6 month intervals. Over the study period there was a steady increase in the number of consults requested and also in the percentage of consults in which rES/rWGS was recommended and ordered by the inpatient genetics consultation service. Dashed line denotes date policy change on May 4, 2022 allowing first tier rES/rWGS for inpatients.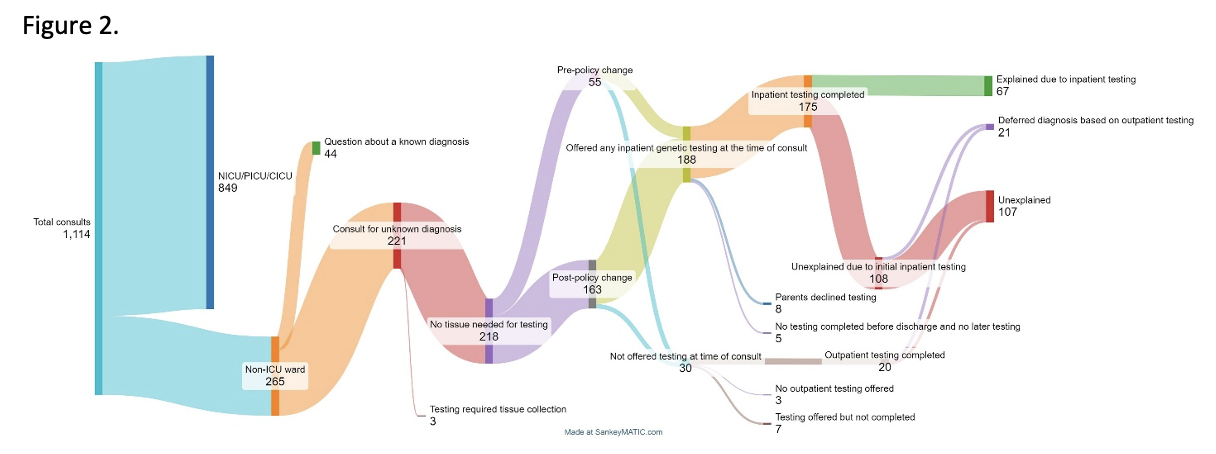 Patients who received genetics consultation from January 1, 2021 through June 30, 2024 included in the present study, testing patterns and outcomes of testing.
Patients who received genetics consultation from January 1, 2021 through June 30, 2024 included in the present study, testing patterns and outcomes of testing.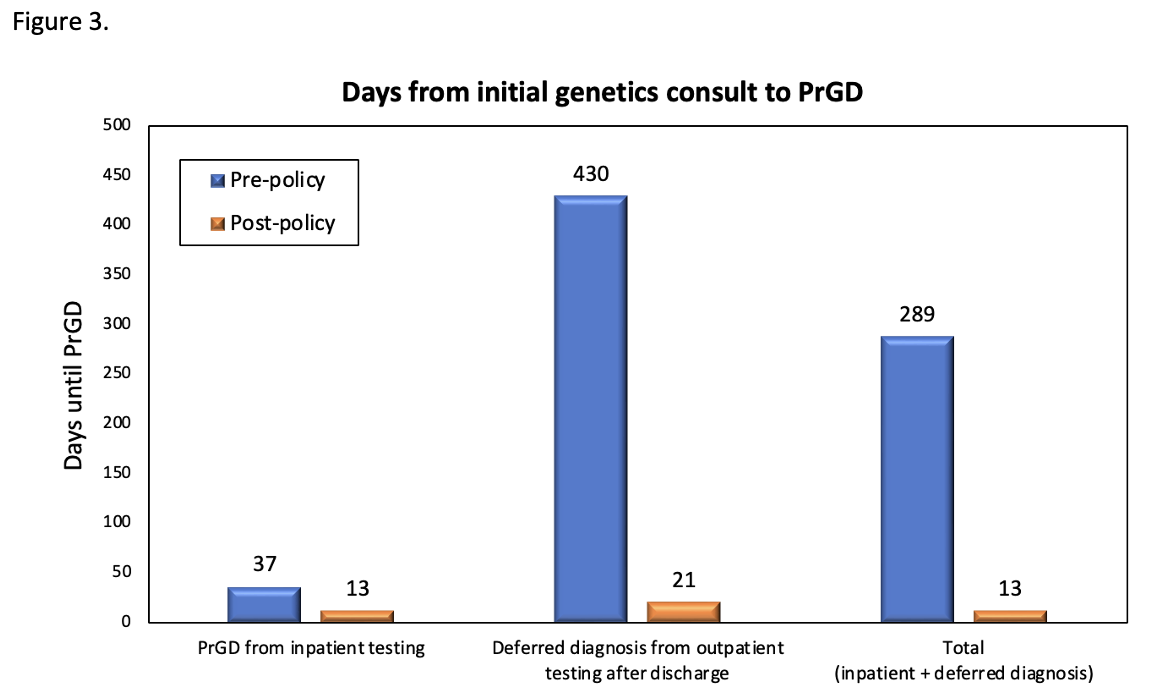 Time to precise genetic diagnosis (PrGD) pre- and post-policy change. Comparisons between time to PrGD from testing sent from the inpatient setting at the time of initial consult, PrGD resulting from testing deferred to the outpatient setting after discharge, and overall time to PrGD for all patients who received inpatient genetics consultation between January 1st, 2021 and June 30, 2024.
Time to precise genetic diagnosis (PrGD) pre- and post-policy change. Comparisons between time to PrGD from testing sent from the inpatient setting at the time of initial consult, PrGD resulting from testing deferred to the outpatient setting after discharge, and overall time to PrGD for all patients who received inpatient genetics consultation between January 1st, 2021 and June 30, 2024.