Neonatal Quality Improvement 3
Session: Neonatal Quality Improvement 3
 Credit")
 photo")
Sarah Kolnik, MD MBA (she/her/hers)
Assitant Professor
University of Washington - Seattle Children's Hospital
Seattle, Washington, United States
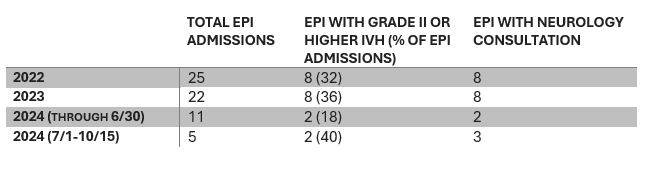
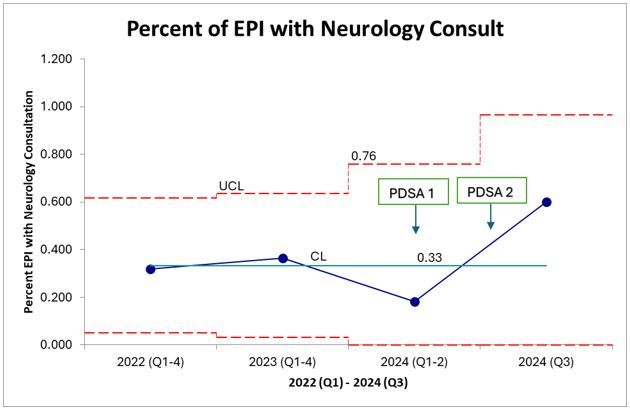 Sixty percent of EPI received neurology consult in Q3 of 2024 after implementation of teleneurology services (PDSA 1) and specification of when to get consult via guideline documentation (PDSA 2), an 80% increase from baseline of 33%.
Sixty percent of EPI received neurology consult in Q3 of 2024 after implementation of teleneurology services (PDSA 1) and specification of when to get consult via guideline documentation (PDSA 2), an 80% increase from baseline of 33%.