
Neonatal Quality Improvement 1
Session: Neonatal Quality Improvement 1
 Credit")
Jennifer B. Fundora, MD
Assistant Professor
Johns Hopkins University School of Medicine
Baltimore, Maryland, United States
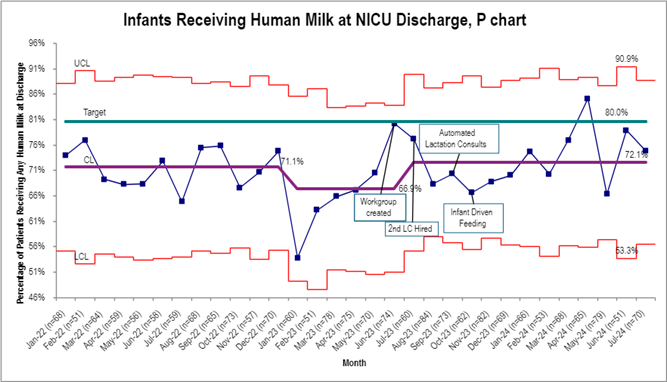 Proportion of infants discharged from the NICU receiving any human milk.
Proportion of infants discharged from the NICU receiving any human milk. 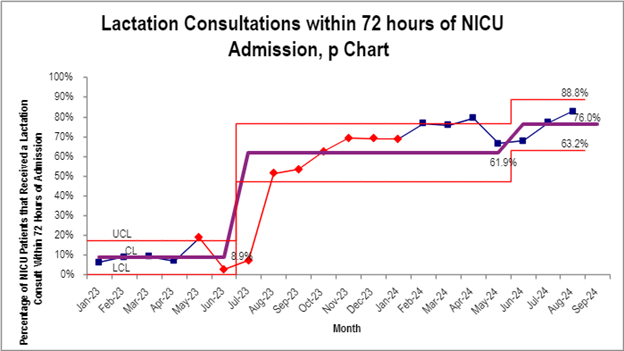 Proportion of infants with lactation visit within 72 hours of admission
Proportion of infants with lactation visit within 72 hours of admission