
Quality Improvement/Patient Safety 2
Session: Quality Improvement/Patient Safety 2
.jpg "Daria Ferro, MD (she/her/hers) photo")
Daria Ferro, MD (she/her/hers)
Attending Physician
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
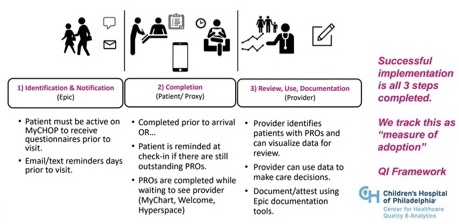 Phase 1 analogous to order for medication/ prescription taking place. Phase 2 analogous to patient/caregiver “filling” med or completing the order. Phase 3 analogous to provider performing “reconciliation.” Our data model tracks each of these three phases to provide insights and potential plan-do-study-act cycles that are independent from one another but synergistically related.
Phase 1 analogous to order for medication/ prescription taking place. Phase 2 analogous to patient/caregiver “filling” med or completing the order. Phase 3 analogous to provider performing “reconciliation.” Our data model tracks each of these three phases to provide insights and potential plan-do-study-act cycles that are independent from one another but synergistically related. 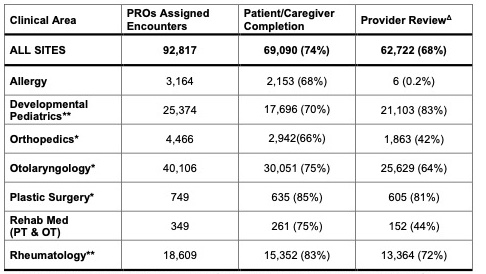 Table 1 represents clinical areas where PROs implementation includes a mechanism for provider documentation for at least 1 full calendar year.
Table 1 represents clinical areas where PROs implementation includes a mechanism for provider documentation for at least 1 full calendar year. 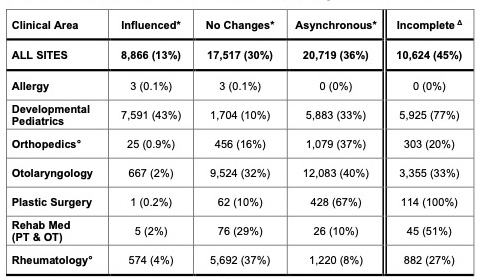 Providers select documentation that maps to four categories:
Providers select documentation that maps to four categories: 