
Neonatal Hemodynamics and Cardiovascular Medicine 1
Session: Neonatal Hemodynamics and Cardiovascular Medicine 1
Valerie Kirtley, MD (she/her/hers)
Resident
Nationwide Children's Hospital
Columbus, Ohio, United States
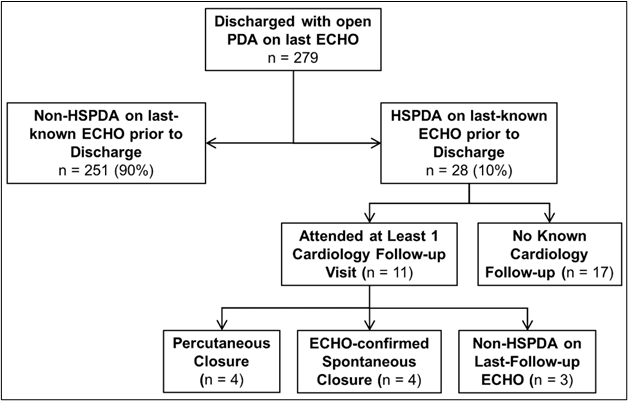 Flowchart showing follow-up incidence and outcomes among 28 extremely preterm infants with a hemodynamically significant patent ductus arteriosus on last-known echocardiogram prior to discharge.Flowchart showing follow-up incidence and outcomes among 28 extremely preterm infants with a hemodynamically significant patent ductus arteriosus on last-known echocardiogram prior to discharge.
Flowchart showing follow-up incidence and outcomes among 28 extremely preterm infants with a hemodynamically significant patent ductus arteriosus on last-known echocardiogram prior to discharge.Flowchart showing follow-up incidence and outcomes among 28 extremely preterm infants with a hemodynamically significant patent ductus arteriosus on last-known echocardiogram prior to discharge.