
Neonatal Neurology 1
Session: Neonatal Neurology 1
 photo")
Kai-Hsiang Hsu, MD (he/him/his)
Associate Professor of Pediatrics
Chang Gung Memorial Hospital, Linkou
Taipei, Taipei, Taiwan (Republic of China)
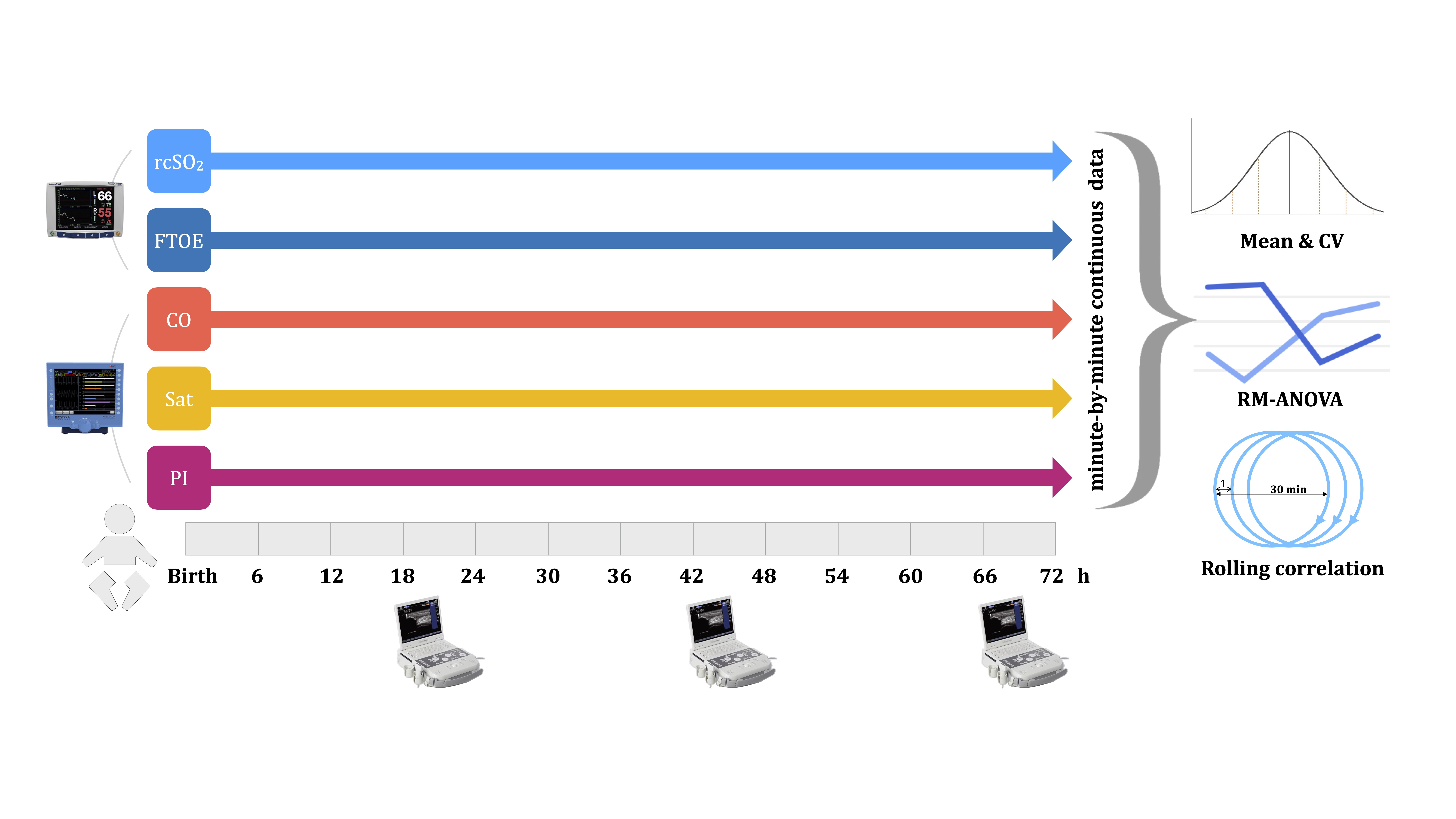 Hemodynamic parameters, including regional cerebral saturation (rcSO₂) , fraction of tissue oxygen extraction (FTOE), cardiac output (CO), arterial saturation (Sat) and perfusion index (PI), were collected minute-by-minute over the first 72 hours. Minute-by-minute data were analyzed between the IVH and non-IVH groups using the mean and coefficient of variation (CV), repeated-measures analysis of variance (RM-ANOVA), and rolling correlations.
Hemodynamic parameters, including regional cerebral saturation (rcSO₂) , fraction of tissue oxygen extraction (FTOE), cardiac output (CO), arterial saturation (Sat) and perfusion index (PI), were collected minute-by-minute over the first 72 hours. Minute-by-minute data were analyzed between the IVH and non-IVH groups using the mean and coefficient of variation (CV), repeated-measures analysis of variance (RM-ANOVA), and rolling correlations.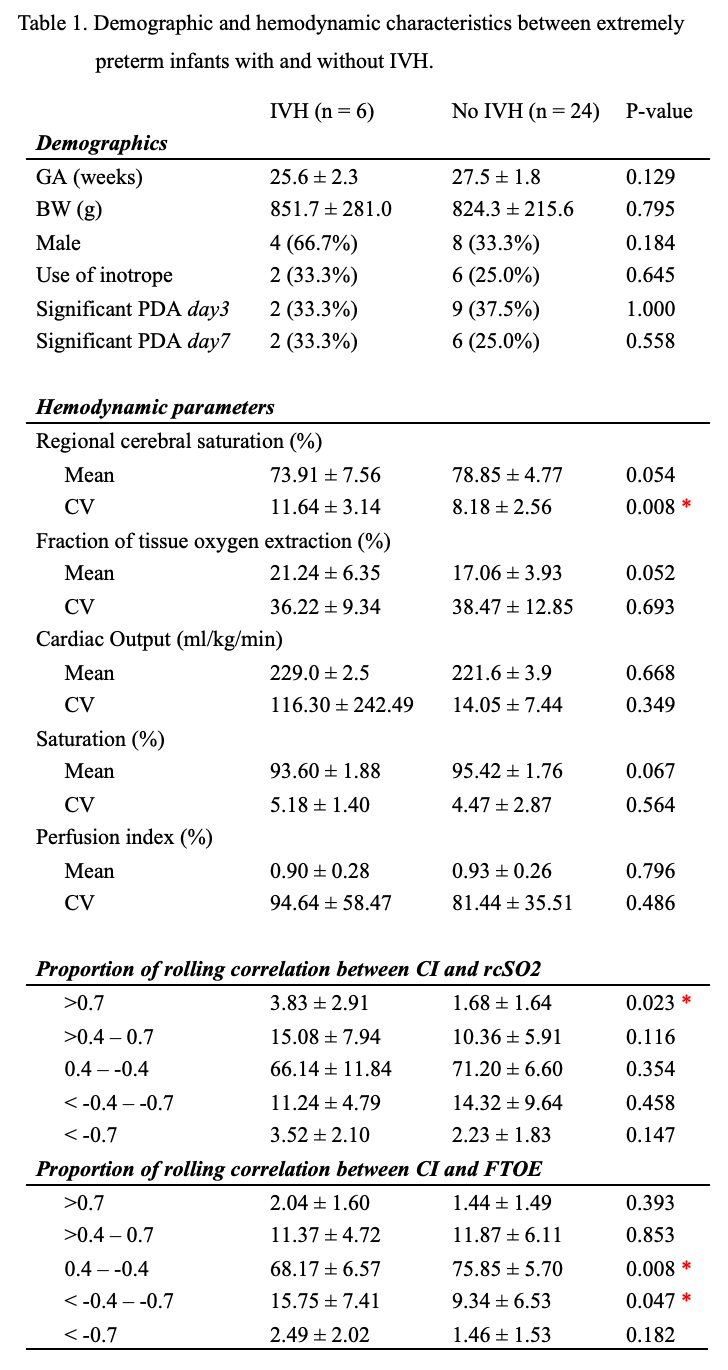 The IVH group exhibited a significantly greater CV of rcSO₂ , more frequent high correlations (r>0.7) in CO–rcSO₂ and less frequent low correlations (r=0.4– -0.7) in CO–FTOE. * indicates statistic significance (p <0.05).
The IVH group exhibited a significantly greater CV of rcSO₂ , more frequent high correlations (r>0.7) in CO–rcSO₂ and less frequent low correlations (r=0.4– -0.7) in CO–FTOE. * indicates statistic significance (p <0.05).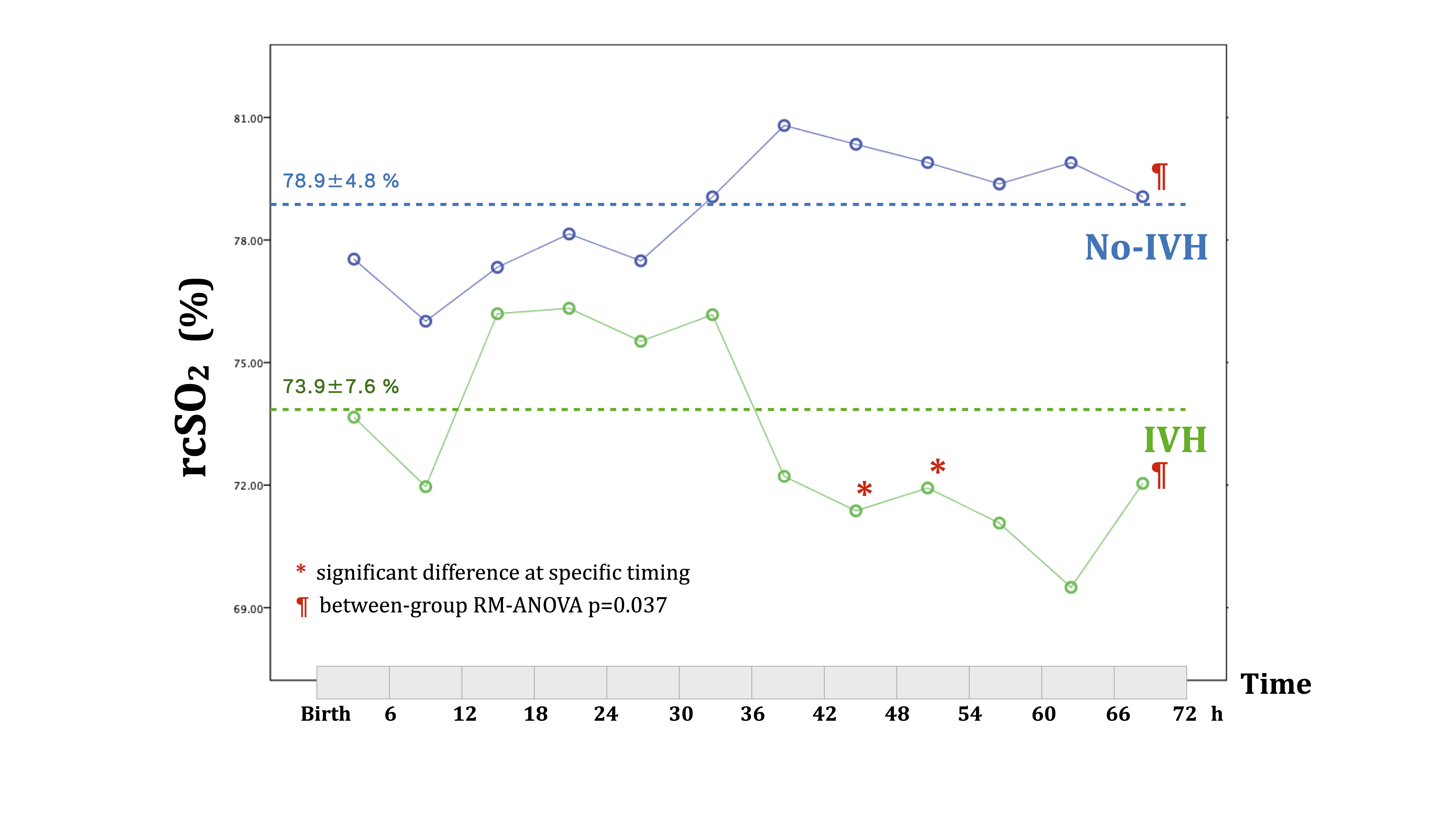 A trend towards lower rcSO₂ was observed in the IVH group (¶ between-group RM-ANOVA p=0.037), particularly after 42 hours of life (*).
A trend towards lower rcSO₂ was observed in the IVH group (¶ between-group RM-ANOVA p=0.037), particularly after 42 hours of life (*).