721 - Jamii ni Afya: Evaluation of a Community Based, Digitally Supported Early Childhood Health and Development Program in Zanzibar
Friday, April 25, 2025
5:30pm - 7:45pm HST
Publication Number: 721.5636
Kim WIlson, Boston Children's Hospital, Wayland, MA, United States; Alina Bhojani, Emory Rollins School of Public Health, Toronto, ON, Canada; Katherine Wright, D-tree International, Grand Rapids, MI, United States; Aisha Abdalla. Mohammed, D-tree Internatioal, Zanzibar, Mjini Magharibi, Tanzania; Salim A. Slim, Ministey of health Zanzibar., zanzibar, Pwani, Tanzania; Kweka A. Hadija, Enhance Tanzania Foundation (ENTAF), Dar es salaam, Dar es Salaam, Tanzania; Julius Rosenhan, Sightsavers, Dar es Salaam, Dar es Salaam, Tanzania; Gibson B. Kagaruki, National Institute for Medical Research (NIMR) - Tanzania, Dar es Salaam, Dar es Salaam, Tanzania; Giulia VR. Besana, London School of Hygiene and Tropical Medicine, Zanzibar, Mjini Magharibi, Tanzania
Boston Children's Hospital Wayland, Massachusetts, United States
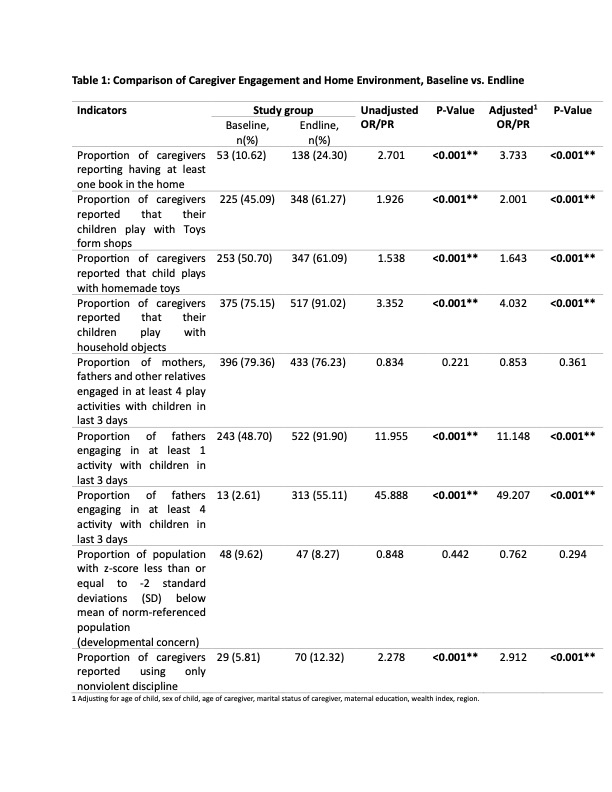
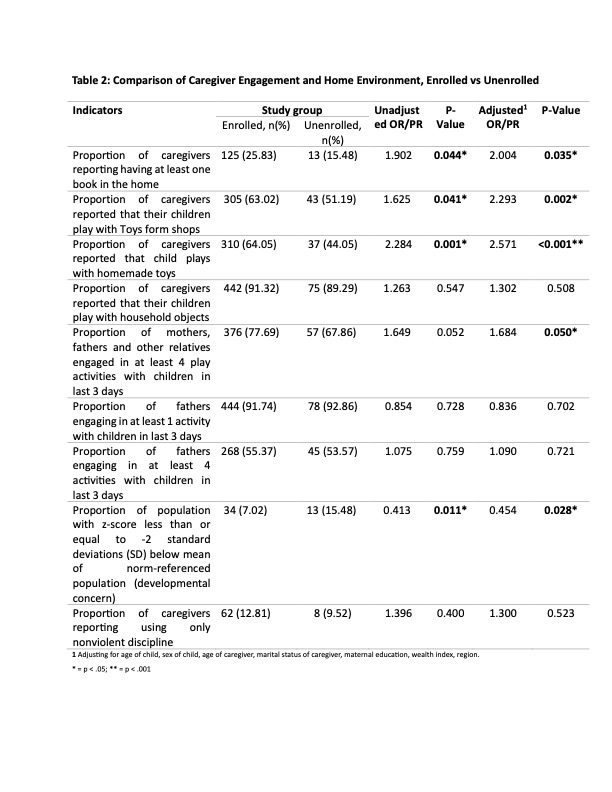
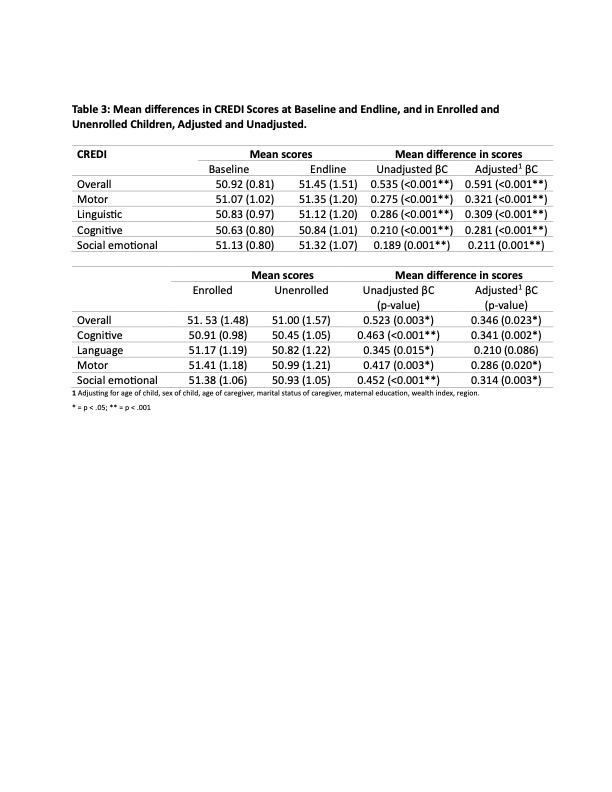
Background: Jamii ni Afya (JNA), a digitally supported community health program in Zanzibar, enrolled over 200,000 children between 2019 and 2023. Community Health Volunteers (CHVs) screened for danger signs, facilitated referrals, and coached caregivers on health, nutrition, responsive parenting, and early learning. Objective: We conducted household surveys aimed at evaluating JNA’s impact. Design/Methods: Nationally representative household surveys were conducted among families with children aged 18 – 29 months in February 2019 (n=499) and December 2023 (n=568). Primary outcomes included the Caregiver Reported Early Developmental Index (CREDI) and established indicators of parenting practices and home environment. We compared outcomes at baseline and endline, and in enrolled vs unenrolled children at endline. Logistic regression was used for binary variables and linear regression for continuous variables. Adjusted models included child age, child sex, caregiver age, maternal marital status, maternal education, wealth index, and region. Results: Compared to baseline, children in the endline survey were more likely to have one or more books (Adjusted OR = 3.73, p< 0.001), play with homemade toys (Adjusted OR = 1.64, p < 0.001), and have fathers engage in at least one play activity (Adjusted OR = 11.15, p< 0.001). There were no significant differences in all caregivers engaging in 4 or more activities (OR = 0.853, p=0.36) (Table 1). At endline, enrolled children were more likely to have one or more books (Adjusted OR= 2.00, p=0.04) and to play with homemade toys (Adjusted OR = 2.57, p < 0.001) vs unenrolled. More caregivers engaged in at least 4 play activities in the enrolled group with marginal statistical significance (Adjusted OR =1.6, p=0.05). There was no significant difference in fathers engaging in play (p=0.70) (Table 2). There was an increase of 0.59 in the adjusted mean CREDI score from baseline to endline (p=0.001) and an increase of 0.35 in mean CREDI in enrolled vs unenrolled children (p = 0.003). An increase in CREDI score was noted in all developmental domains, except for the adjusted language model in enrolled children (Table 3).
Conclusion(s): Home environment, caregiver engagement, and child developmental outcomes improved from baseline to end-line, and in comparison between enrolled vs unenrolled children following JNA's implementation of a holistic community health home visiting program targeting optimal health, nutrition, responsive parenting, and early learning in families with young children in Zanzibar.
Table 1: Caregiver Engagement and Home Environment Baseline vs. Endline
Table 2: Caregiver Engagement and Home Environment, Enrolled vs. Unenrolled
Table 3: Mean Differences in CREDI Scores, Baseline vs. Endline and Enrolled vs. Unenrolled
Table 1: Caregiver Engagement and Home Environment Baseline vs. Endline
Table 2: Caregiver Engagement and Home Environment, Enrolled vs. Unenrolled
Table 3: Mean Differences in CREDI Scores, Baseline vs. Endline and Enrolled vs. Unenrolled