
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
 Credit")

Wissam Shalish, MD, PhD
Neonatologist
McGill University Faculty of Medicine and Health Sciences
Montreal, Quebec, United States
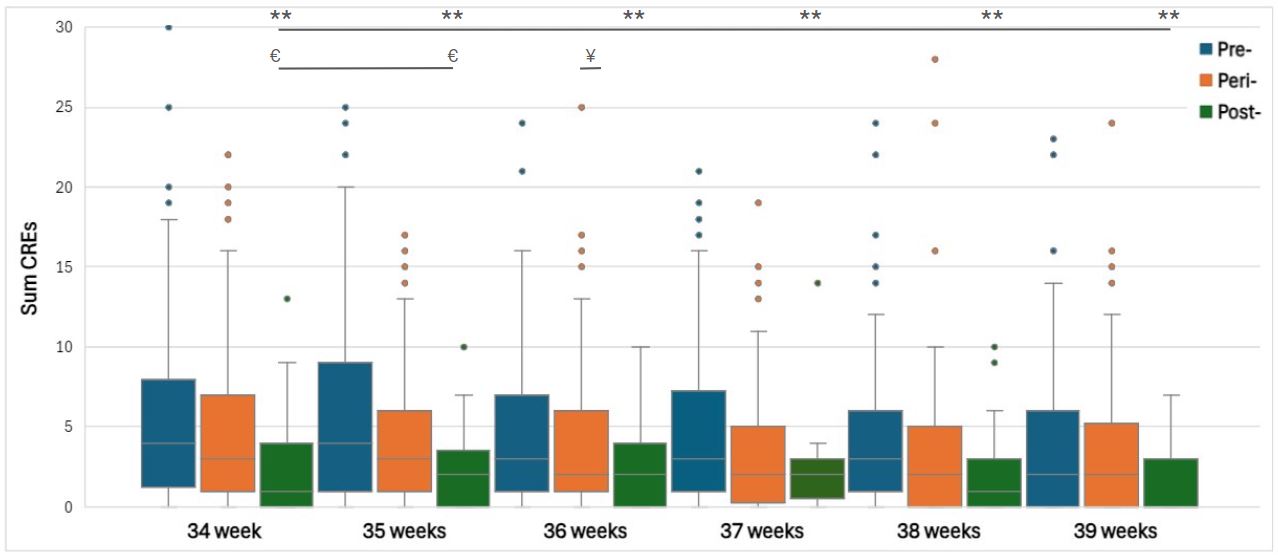 Legend: ¥; p <0.05 comparing pre- vs. peri-caffeine protocol, €; p <0.05 comparing peri- vs. post-caffeine protocol, **; p <0.05 comparing post- vs. pre-caffeine protocol. CREs (cardiorespiratory events) were defined as any nurse-recorded apneas, bradycardias, or desaturations requiring tactile stimulation, supplemental oxygen, and/or bag-mask ventilation.
Legend: ¥; p <0.05 comparing pre- vs. peri-caffeine protocol, €; p <0.05 comparing peri- vs. post-caffeine protocol, **; p <0.05 comparing post- vs. pre-caffeine protocol. CREs (cardiorespiratory events) were defined as any nurse-recorded apneas, bradycardias, or desaturations requiring tactile stimulation, supplemental oxygen, and/or bag-mask ventilation. 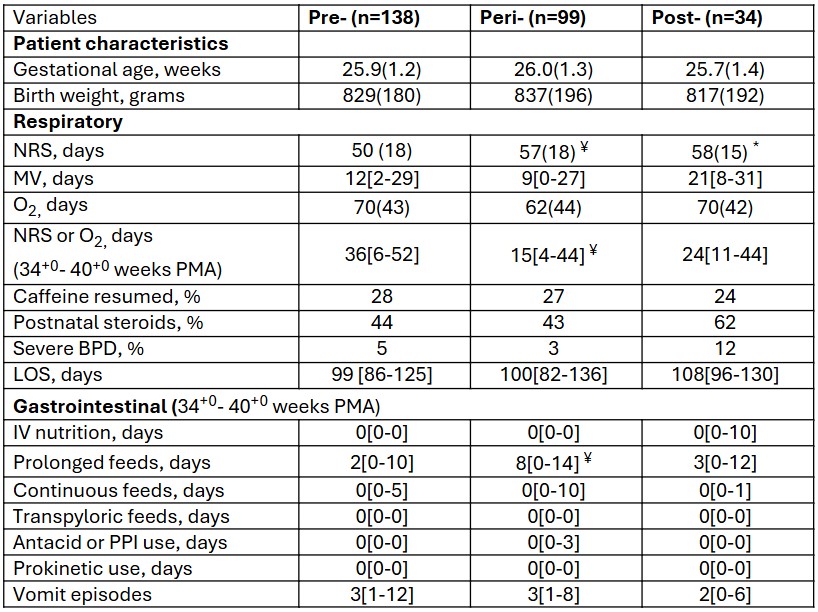 Abbreviations: BPD; bronchopulmonary dysplasia, LOS; length of stay, MV; mechanical ventilation, NRS; non-invasive respiratory support, O2; supplemental oxygen, PMA; postmenstrual age, PPI; proton pump inhibitor
Abbreviations: BPD; bronchopulmonary dysplasia, LOS; length of stay, MV; mechanical ventilation, NRS; non-invasive respiratory support, O2; supplemental oxygen, PMA; postmenstrual age, PPI; proton pump inhibitor 