
Neonatal/Infant Resuscitation 2
Session: Neonatal/Infant Resuscitation 2
 photo")
Manoj Biniwale, MD (he/him/his)
Director of NICU Clinical Research
Cedars Sinai Medical Canter
Los Angeles, California, United States
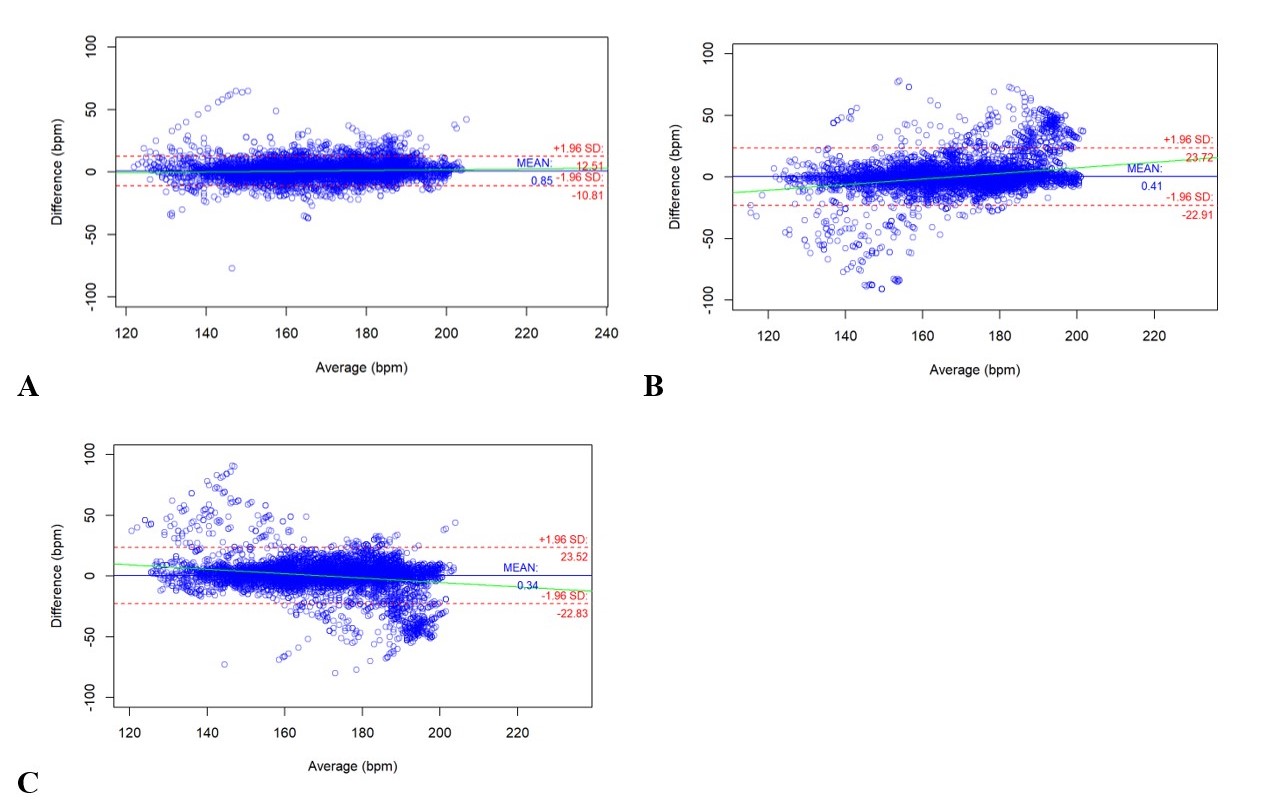 x-axis represents heart rate and the y-axis represents difference in reading between devices.
x-axis represents heart rate and the y-axis represents difference in reading between devices..jpg) The x-axis represents SpO2 (%) and the y-axis represents difference in reading between devices.
The x-axis represents SpO2 (%) and the y-axis represents difference in reading between devices. 