
Neonatal Neurology 1
Session: Neonatal Neurology 1
Jessie Ting Guo, PhD
Senior Research Associate
The Hospital for Sick Children
Toronto, Ontario, Canada
.png)
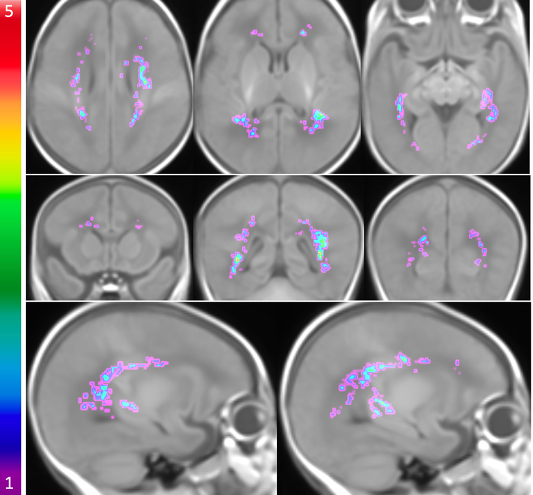 The probabilistic WMI map of 40 MLP infants overlaid on the brain template displayed on axial planes (superior to inferior), coronal planes (anterior to posterior), and sagittal planes (left to right). The colour bar on the left indicates the colour coding of the WMI summation where WMI occurs at homologous regions across the MLP infants.
The probabilistic WMI map of 40 MLP infants overlaid on the brain template displayed on axial planes (superior to inferior), coronal planes (anterior to posterior), and sagittal planes (left to right). The colour bar on the left indicates the colour coding of the WMI summation where WMI occurs at homologous regions across the MLP infants.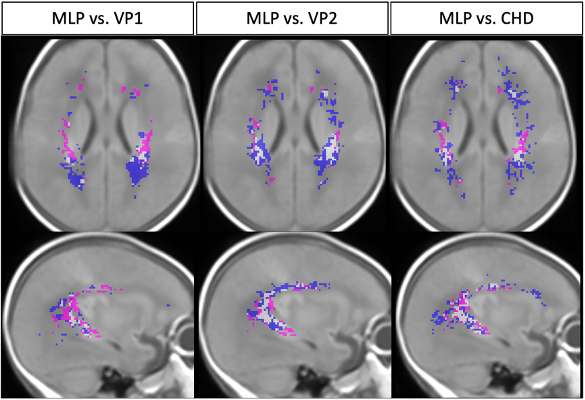 Comparison of WMI identified in 40 MLP infants at early-life or TEA with WMI in 68 very preterm infants from VP-cohort 1 (1st column) and in 58 very preterm infants from VP-cohort 2 (2nd column) at early-life, as well as with WMI in 86 term CHD infants (3rd column) on an axial plane and a sagittal plane of the brain template. Magenta: WMI identified only in MLP infants; Blue: WMI only in VP-cohort 1, VP-cohort 2 or CHD infants; White: WMI that are common in MLP and any other cohort.
Comparison of WMI identified in 40 MLP infants at early-life or TEA with WMI in 68 very preterm infants from VP-cohort 1 (1st column) and in 58 very preterm infants from VP-cohort 2 (2nd column) at early-life, as well as with WMI in 86 term CHD infants (3rd column) on an axial plane and a sagittal plane of the brain template. Magenta: WMI identified only in MLP infants; Blue: WMI only in VP-cohort 1, VP-cohort 2 or CHD infants; White: WMI that are common in MLP and any other cohort.