
Neonatal/Infant Resuscitation 1
Session: Neonatal/Infant Resuscitation 1

Stephanie De Ocampo, MSN
Registered Nurse
Kaiser Foundation Hospital - Roseville Women's and Children's Services
Roseville, California, United States
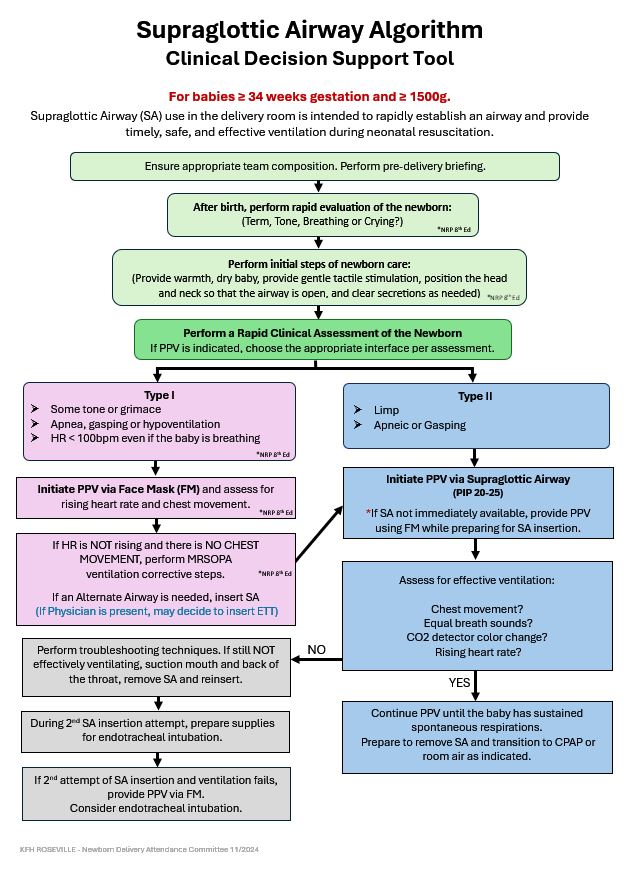 Figure 1: Supraglottic Airway Algorithm: Clinical Decision Support Tool
Figure 1: Supraglottic Airway Algorithm: Clinical Decision Support Tool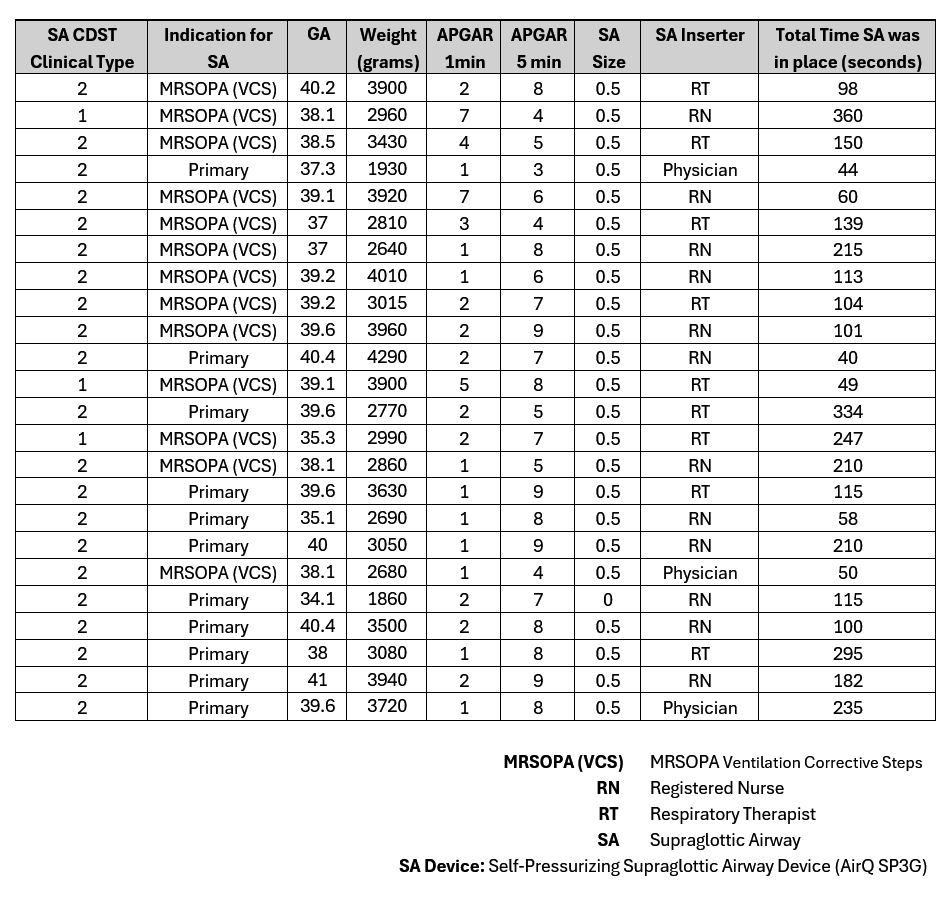 Table 1: Supraglottic Airway Insertion ReportFigure 1: Supraglottic Airway Algorithm: Clinical Decision Support ToolTable 1: Supraglottic Airway Insertion Report
Table 1: Supraglottic Airway Insertion ReportFigure 1: Supraglottic Airway Algorithm: Clinical Decision Support ToolTable 1: Supraglottic Airway Insertion Report