
Neonatal Pulmonology - Clinical 2: BPD: Incidence, Treatment, Outcomes
Session: Neonatal Pulmonology - Clinical 2: BPD: Incidence, Treatment, Outcomes
Rakesh Lavu, MD
Fellow
Cleveland Clinic Children's
Beachwood, Ohio, United States
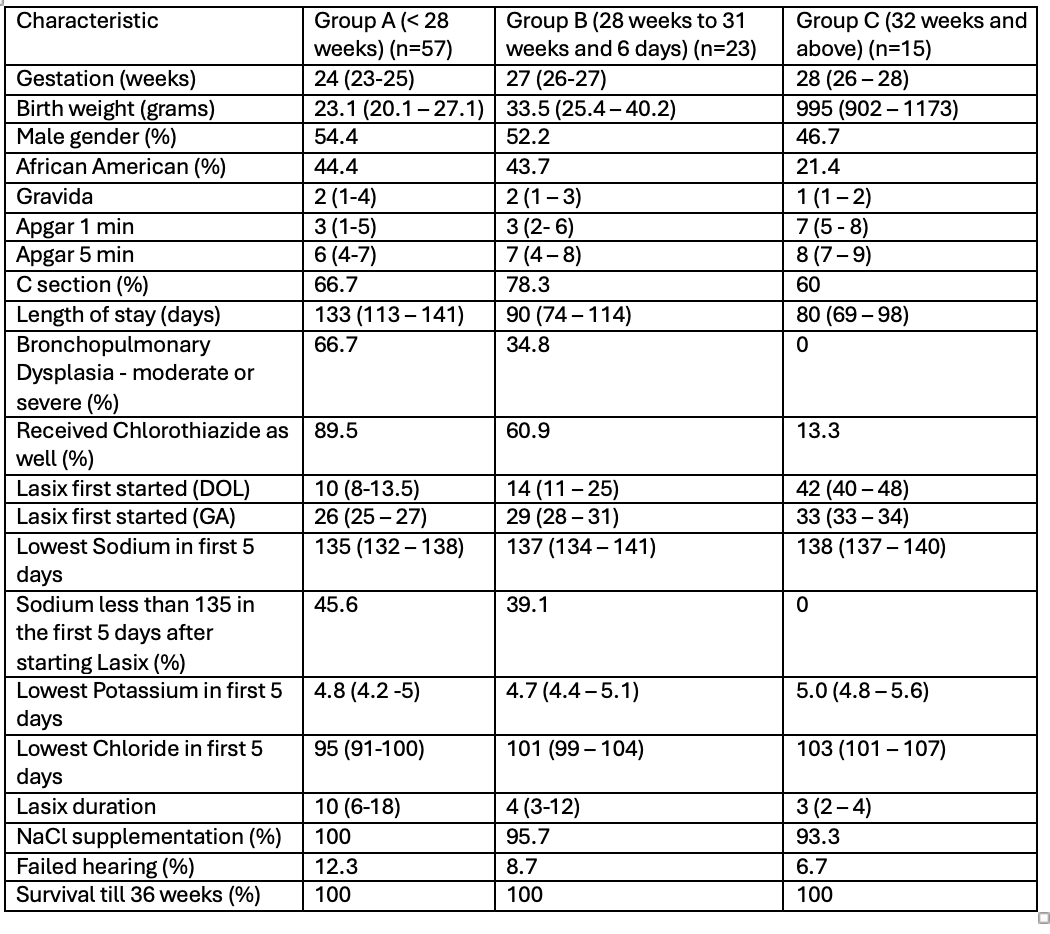 Demographic characteristics, primary and secondary outcome of the population
Demographic characteristics, primary and secondary outcome of the population.png) Boxplot diagram showing the lowest Sodium and Potassium levels within 5 days after starting furosemide in the three GA groups: < 28 weeks, 28-31 weeks, and 32 weeks or more.
Boxplot diagram showing the lowest Sodium and Potassium levels within 5 days after starting furosemide in the three GA groups: < 28 weeks, 28-31 weeks, and 32 weeks or more.