
Neonatal/Infant Resuscitation 1
Session: Neonatal/Infant Resuscitation 1
 photo")
Kirsten A. Gilliland, MD (she/her/hers)
Resident
Children's Hospital Colorado
Denver, Colorado, United States
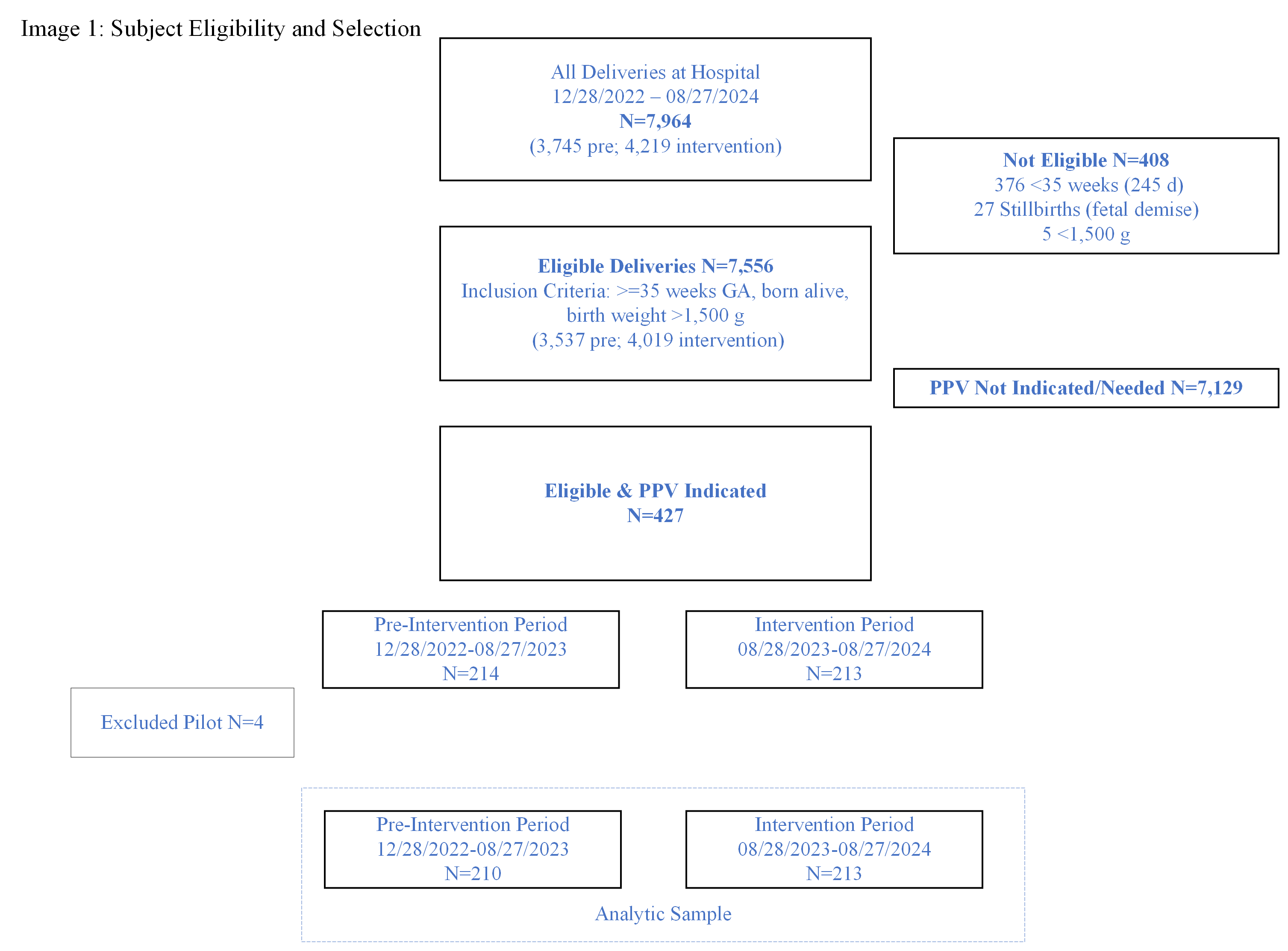 This image depicts the selection criteria for the study and final sample for the pre-intervention and intervention periods.
This image depicts the selection criteria for the study and final sample for the pre-intervention and intervention periods. 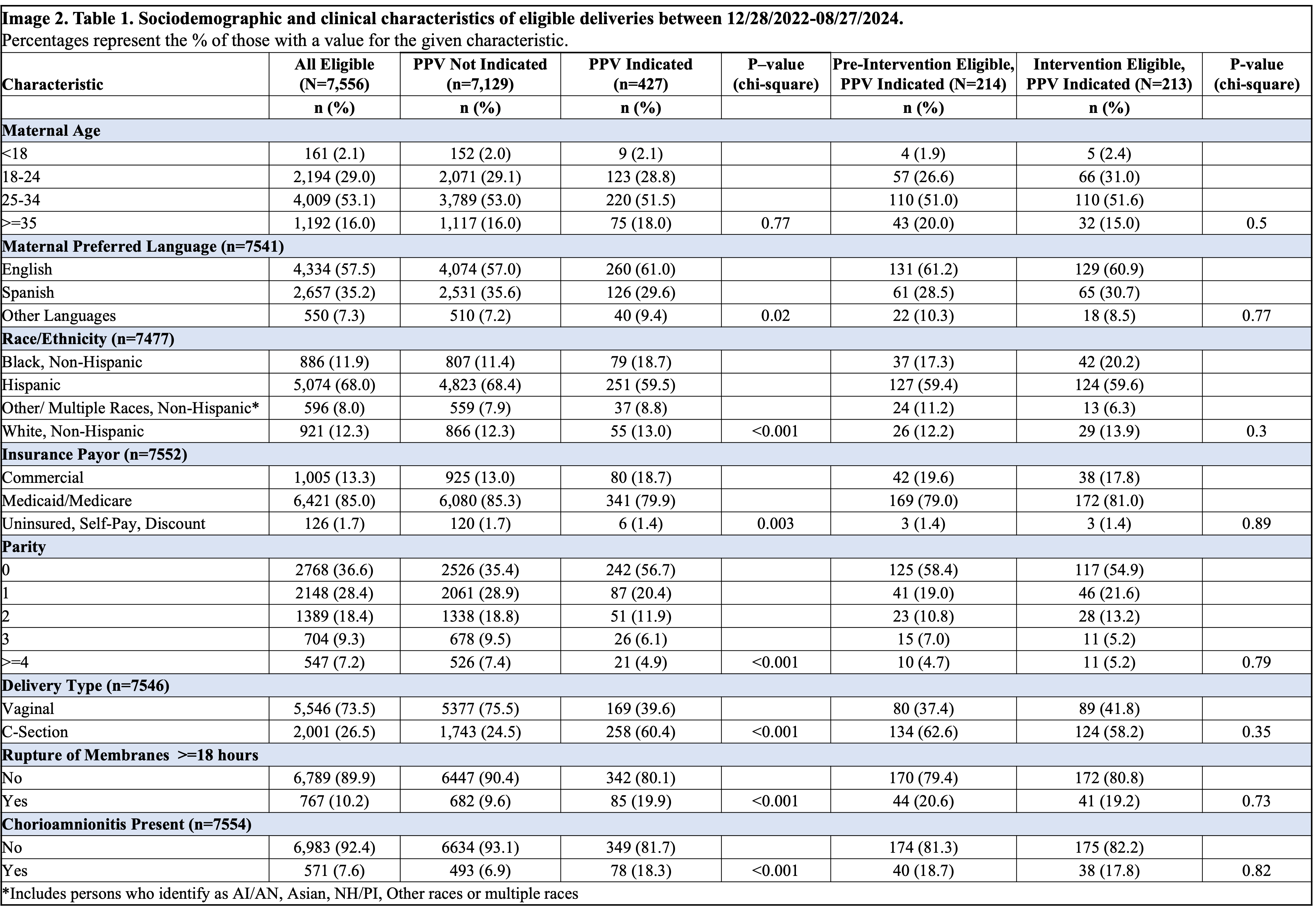 In comparing pre-intervention eligible and intervention eligible groups, there are no significant differences.
In comparing pre-intervention eligible and intervention eligible groups, there are no significant differences..png) There is a statistically significant (p < 0.001) difference in providers using LMA only or as first-line with 1 minute APGAR scored 0-3 in the intervention period. Otherwise, there are no statistically significant differences with FM use compared to LMA use for PPV in the analyzed outcomes (5 and 10 minute APGAR scores, NICU admission, intubation, chest compressions, epinephrine use, and HIE).
There is a statistically significant (p < 0.001) difference in providers using LMA only or as first-line with 1 minute APGAR scored 0-3 in the intervention period. Otherwise, there are no statistically significant differences with FM use compared to LMA use for PPV in the analyzed outcomes (5 and 10 minute APGAR scores, NICU admission, intubation, chest compressions, epinephrine use, and HIE). 