
Global Neonatal & Children's Health 1
Session: Global Neonatal & Children's Health 1

David Hendrixson, MD
Assistant Professor
University of Washington School of Medicine
Seattle, Washington, United States
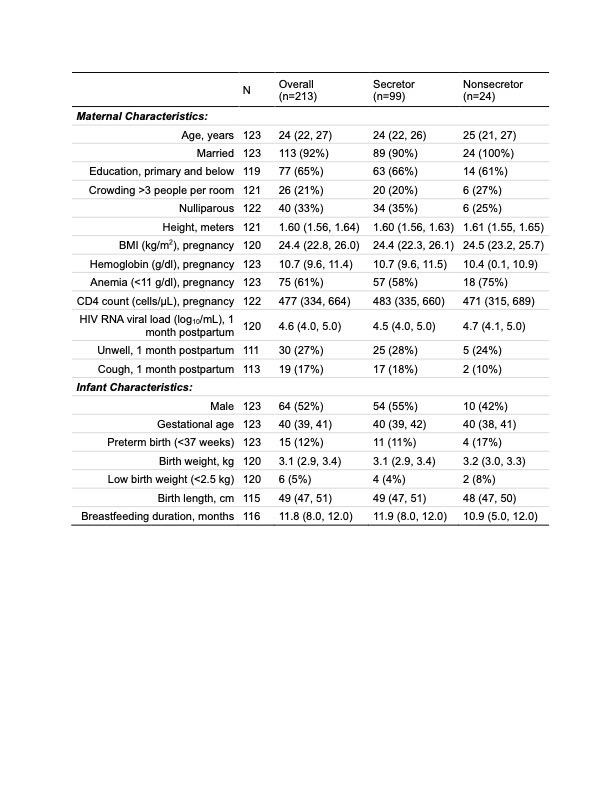 Values expressed as n(%) or median (quartile 1, quartile 3)
Values expressed as n(%) or median (quartile 1, quartile 3).jpg) 1Incidence of diarrhea, allowing repeat episodes with a 14-day window for new episodes
1Incidence of diarrhea, allowing repeat episodes with a 14-day window for new episodes 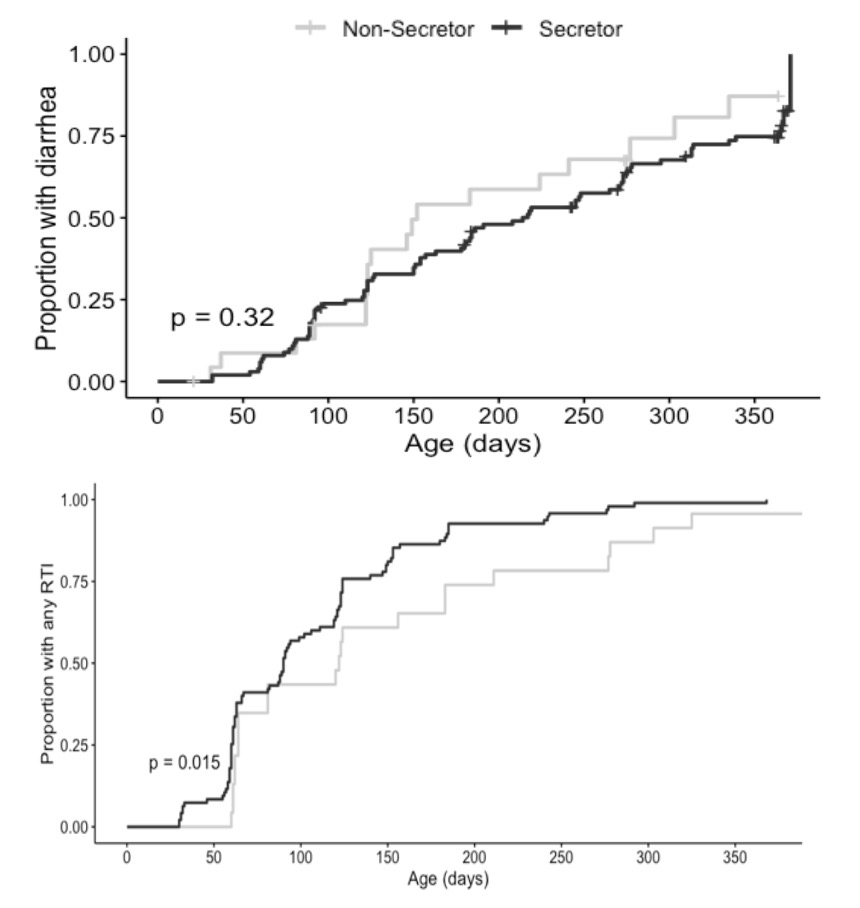 Values expressed as n(%) or median (quartile 1, quartile 3)1Incidence of diarrhea, allowing repeat episodes with a 14-day window for new episodes
Values expressed as n(%) or median (quartile 1, quartile 3)1Incidence of diarrhea, allowing repeat episodes with a 14-day window for new episodes 