
Neonatal Neurology 1
Session: Neonatal Neurology 1
 photo")
Kristen Coletti, MD (she/her/hers)
Neonatologist
Childrens Hospital of Philadelphia
Wynnewood, Pennsylvania, United States
.png) Rates, timing and type of neurosurgical interventions for PHVD over time. (A) Postnatal age at first surgical intervention overall and stratified by primary surgery type (TD or PS); (B) Post-menstrual age at first surgical intervention overall and stratified by primary surgery type (TD or PS); (C) Rate of surgical intervention for PHVD over time overall and stratified by primary surgery type (TD or PS); (D) Rate of conversion from TD to PS over time among infants with primary TD. TD, temporizing device; PS, permanent shunt.
Rates, timing and type of neurosurgical interventions for PHVD over time. (A) Postnatal age at first surgical intervention overall and stratified by primary surgery type (TD or PS); (B) Post-menstrual age at first surgical intervention overall and stratified by primary surgery type (TD or PS); (C) Rate of surgical intervention for PHVD over time overall and stratified by primary surgery type (TD or PS); (D) Rate of conversion from TD to PS over time among infants with primary TD. TD, temporizing device; PS, permanent shunt..png) * Adjusted Odds ratio (95% CI) for categorical outcomes were obtained using Logistic regression. Parameter estimates (95% CI) for continuous outcomes were obtained using generalized linear model. All models were adjusted for gestational age, gender, race and antenatal steroids. The odds ratio and parameter estimates compare Early Intervention vs. Late Intervention.
* Adjusted Odds ratio (95% CI) for categorical outcomes were obtained using Logistic regression. Parameter estimates (95% CI) for continuous outcomes were obtained using generalized linear model. All models were adjusted for gestational age, gender, race and antenatal steroids. The odds ratio and parameter estimates compare Early Intervention vs. Late Intervention.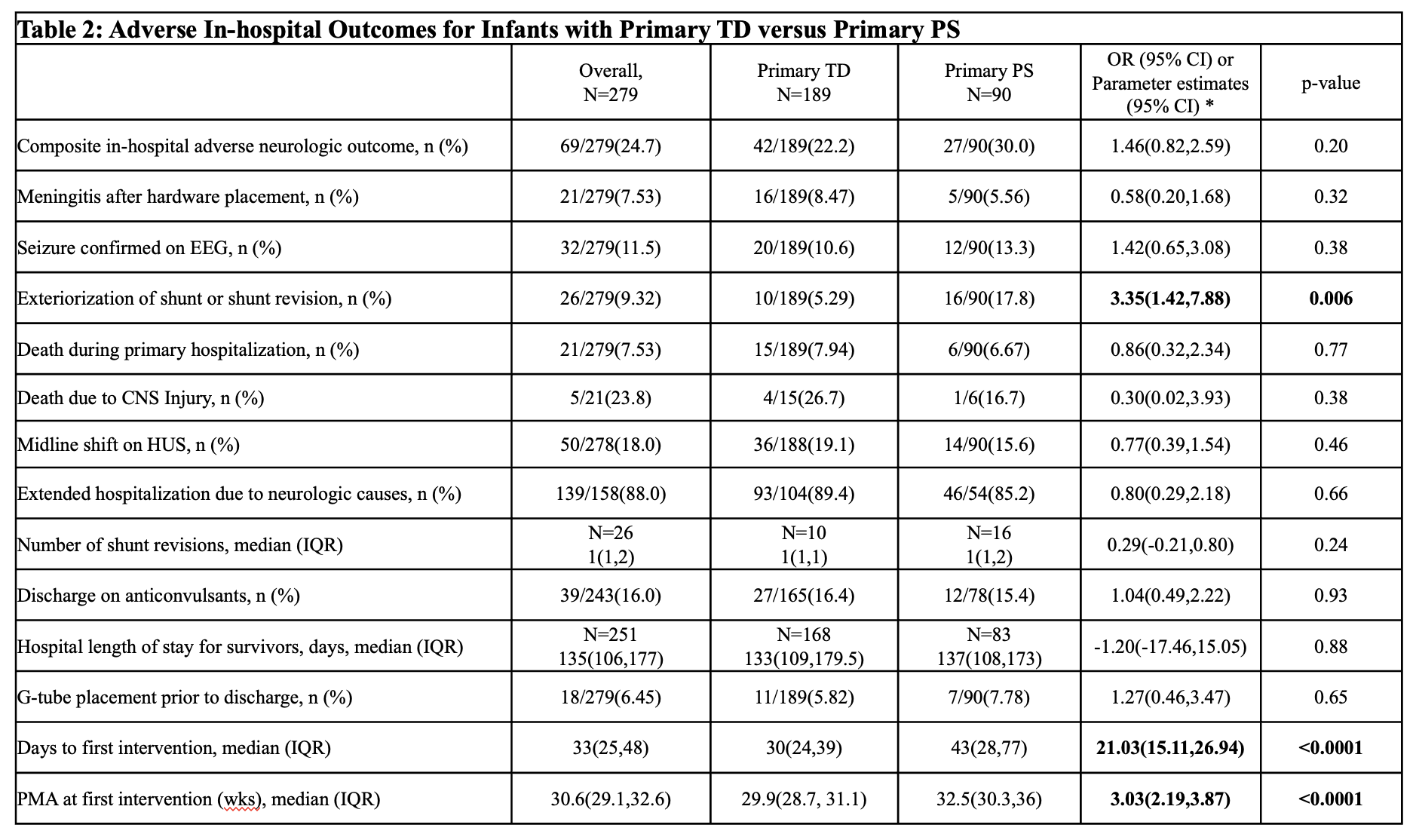 * Adjusted Odds ratio (95% CI) for categorical outcomes were obtained using Logistic regression. Parameter estimates (95% CI) for continuous outcomes were obtained using generalized linear model. All models were adjusted for gestational age, birth weight, gender, and race. The odds ratio and parameter estimates compare Primary PS vs. Primary TD.
* Adjusted Odds ratio (95% CI) for categorical outcomes were obtained using Logistic regression. Parameter estimates (95% CI) for continuous outcomes were obtained using generalized linear model. All models were adjusted for gestational age, birth weight, gender, and race. The odds ratio and parameter estimates compare Primary PS vs. Primary TD.