
Neonatal/Infant Resuscitation 2
Session: Neonatal/Infant Resuscitation 2
Graeme Polglase, PhD (he/him/his)
Professor, Deputy Centre Head
Monash University
Melbourne, Victoria, Australia
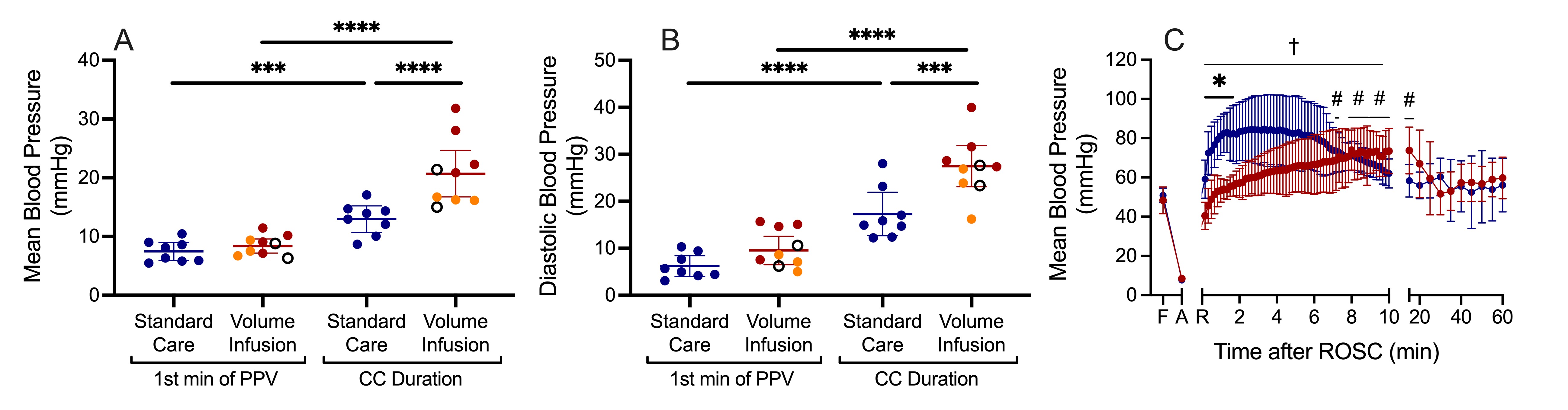 Figure 1: A) Mean and B) Diastolic blood pressure during the first minute of positive pressure ventilation and throughout chest compressions in Standard Care (blue) and Volume Infusion (red) lambs. Note, Volume Infusion lambs in orange required rescue Epinephrine and open circles represent lambs that did not achieve ROSC. C) Mean blood pressure after ROSC – note the overshoot of blood pressure in Standard Care lambs.
Figure 1: A) Mean and B) Diastolic blood pressure during the first minute of positive pressure ventilation and throughout chest compressions in Standard Care (blue) and Volume Infusion (red) lambs. Note, Volume Infusion lambs in orange required rescue Epinephrine and open circles represent lambs that did not achieve ROSC. C) Mean blood pressure after ROSC – note the overshoot of blood pressure in Standard Care lambs.