
Global Neonatal & Children's Health 1
Session: Global Neonatal & Children's Health 1
 photo")
Samantha M. Langer, MD, FAAP (she/her/hers)
Pediatric Emergency Medicine Fellow
Icahn School of Medicine at Mount Sinai
New York, New York, United States
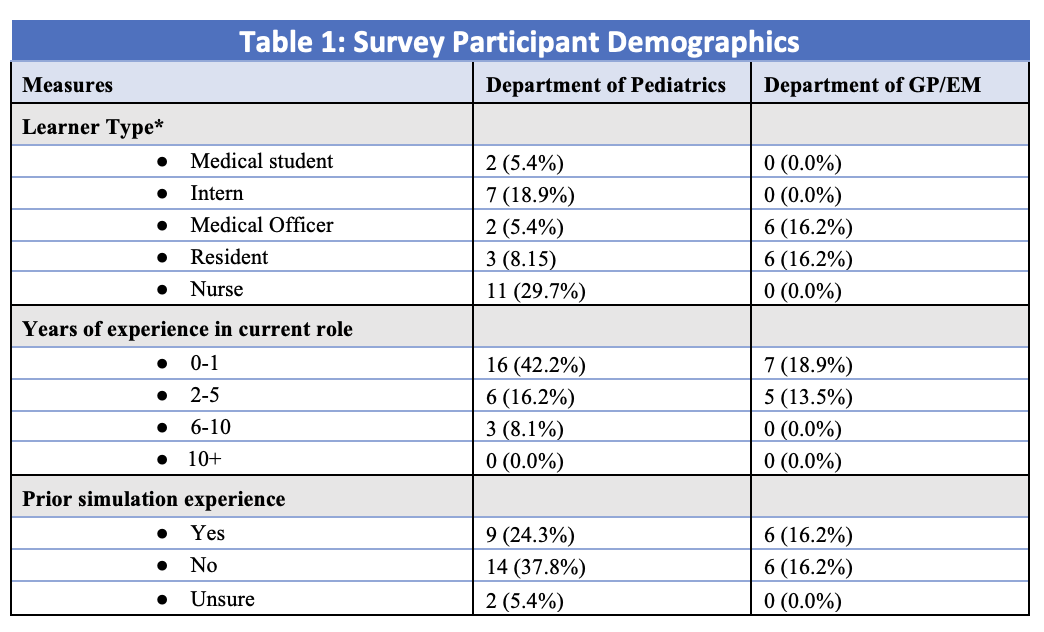 *The medical education process in Nepal differs from that in the US. Medical school is 5 years, followed by a 1-year internship. After passing a general licensing exam, they become a Medical Officer for 1-2 years, followed by an additional board exam. After passing the board exam, they can then apply to and complete a specialty specific 3- year residency program.
*The medical education process in Nepal differs from that in the US. Medical school is 5 years, followed by a 1-year internship. After passing a general licensing exam, they become a Medical Officer for 1-2 years, followed by an additional board exam. After passing the board exam, they can then apply to and complete a specialty specific 3- year residency program. 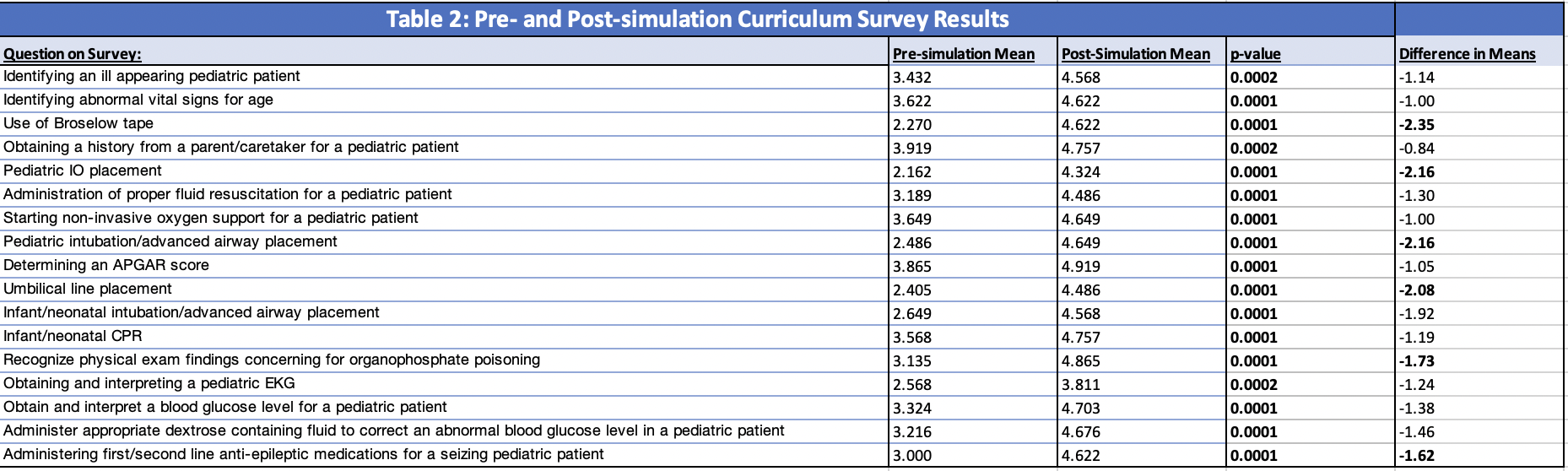 The surveys included a list of procedures and scenarios and asked participants to rate their confidence level on a scale of 1-6 (1 = no confidence/never performed, 6 = high confidence/expert level). T-test analysis of mean survey responses with respect to both pre- and post-simulation provider task comfort levels is reported with the corresponding task listed. Tasks that demonstrated statistically significant improvement in provider comfort level following simulation are bolded with a p-value < 0.05. Additionally, the differences in pre-simulation to post-simulation means are reported, with those questions showing a relative delta of > 1.50 are bolded.
The surveys included a list of procedures and scenarios and asked participants to rate their confidence level on a scale of 1-6 (1 = no confidence/never performed, 6 = high confidence/expert level). T-test analysis of mean survey responses with respect to both pre- and post-simulation provider task comfort levels is reported with the corresponding task listed. Tasks that demonstrated statistically significant improvement in provider comfort level following simulation are bolded with a p-value < 0.05. Additionally, the differences in pre-simulation to post-simulation means are reported, with those questions showing a relative delta of > 1.50 are bolded. 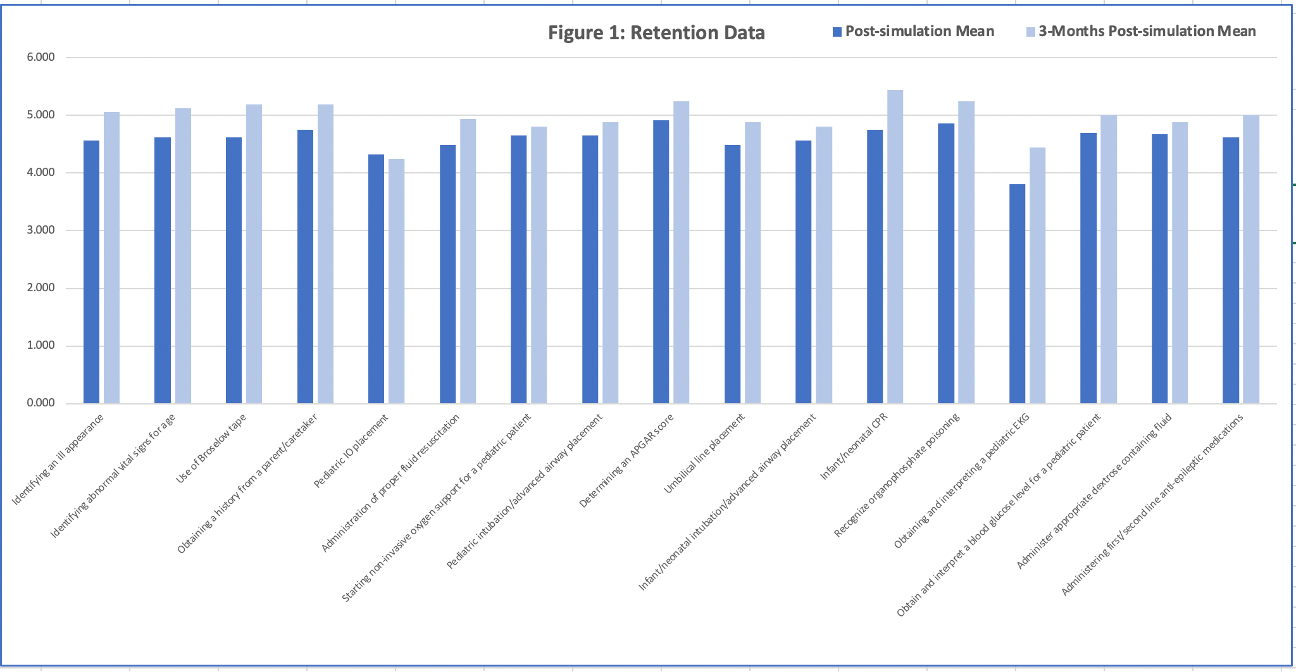 This figure compares the average provider task comfort levels for each question on the post-simulation survey completed immediately after the course with the 3-month post-simulation survey which was later sent to participants to assess long-term retention. All questions showed an equal or great score on the 3-month survey, with the exception of pediatric IO placement, as shown above. Post-simulation survey had a total of 37 responses and the 3-month retention survey had 16 responses.
This figure compares the average provider task comfort levels for each question on the post-simulation survey completed immediately after the course with the 3-month post-simulation survey which was later sent to participants to assess long-term retention. All questions showed an equal or great score on the 3-month survey, with the exception of pediatric IO placement, as shown above. Post-simulation survey had a total of 37 responses and the 3-month retention survey had 16 responses.