
Neonatal Neurology 2
Session: Neonatal Neurology 2
Li-Wen Chen, MD PhD (she/her/hers)
Attending Physician
National Cheng Kung Univertisy Hospital
Tainan, Tainan, Taiwan (Republic of China)
.jpg) Differences in the developmental trajectory of cognition (A), language (B), and motor (C) performance from corrected age 6 months, 12 months to 24 months among the three neurodevelopmental impairment (NDI) outcome groups of extremely preterm infants without severe neonatal brain injury.
Differences in the developmental trajectory of cognition (A), language (B), and motor (C) performance from corrected age 6 months, 12 months to 24 months among the three neurodevelopmental impairment (NDI) outcome groups of extremely preterm infants without severe neonatal brain injury. 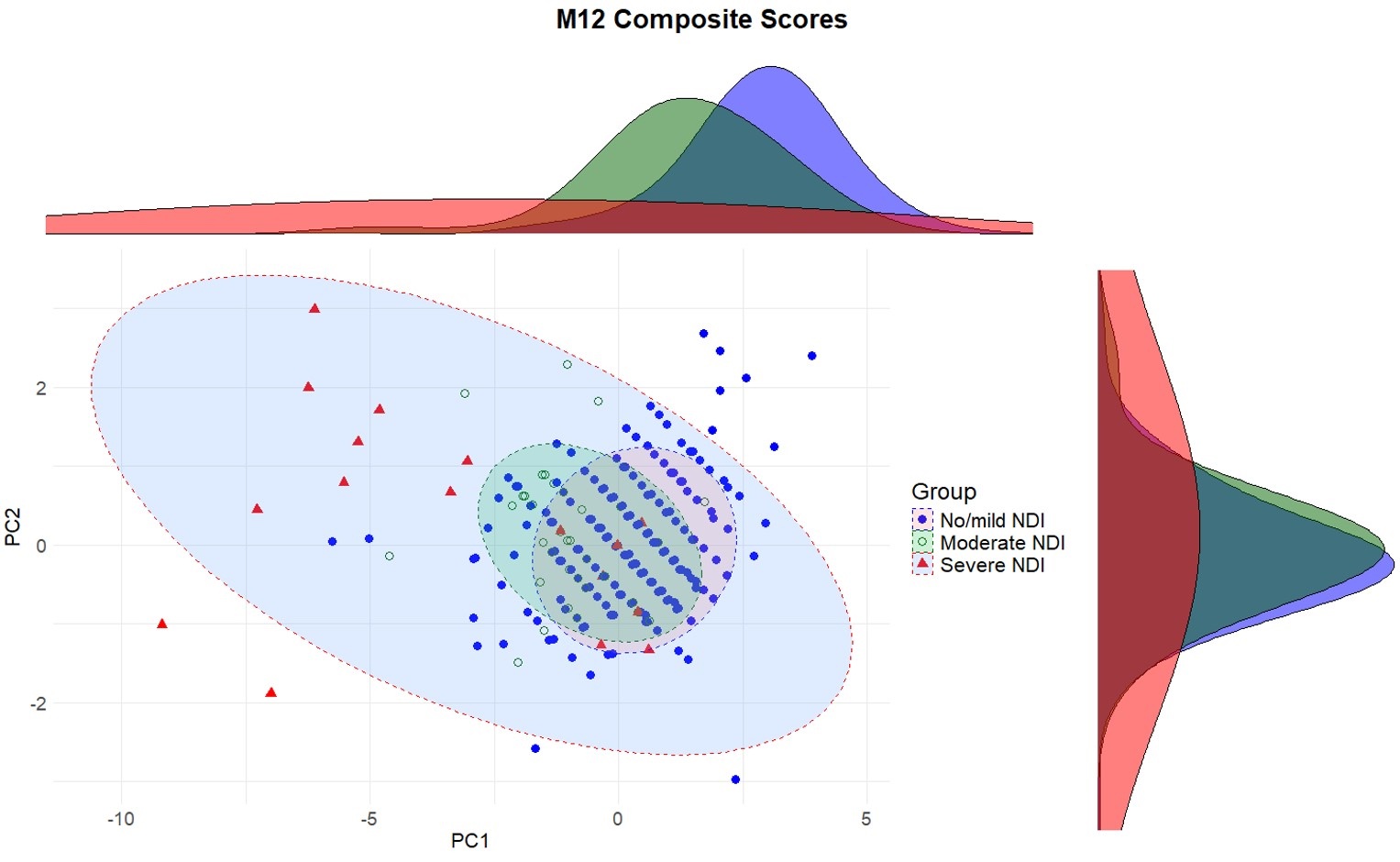 Principal component (PC) analysis using cognitive, language, and motor developmental performances at age 12 months (M12) for NDI outcomes at 24 months of age.
Principal component (PC) analysis using cognitive, language, and motor developmental performances at age 12 months (M12) for NDI outcomes at 24 months of age. 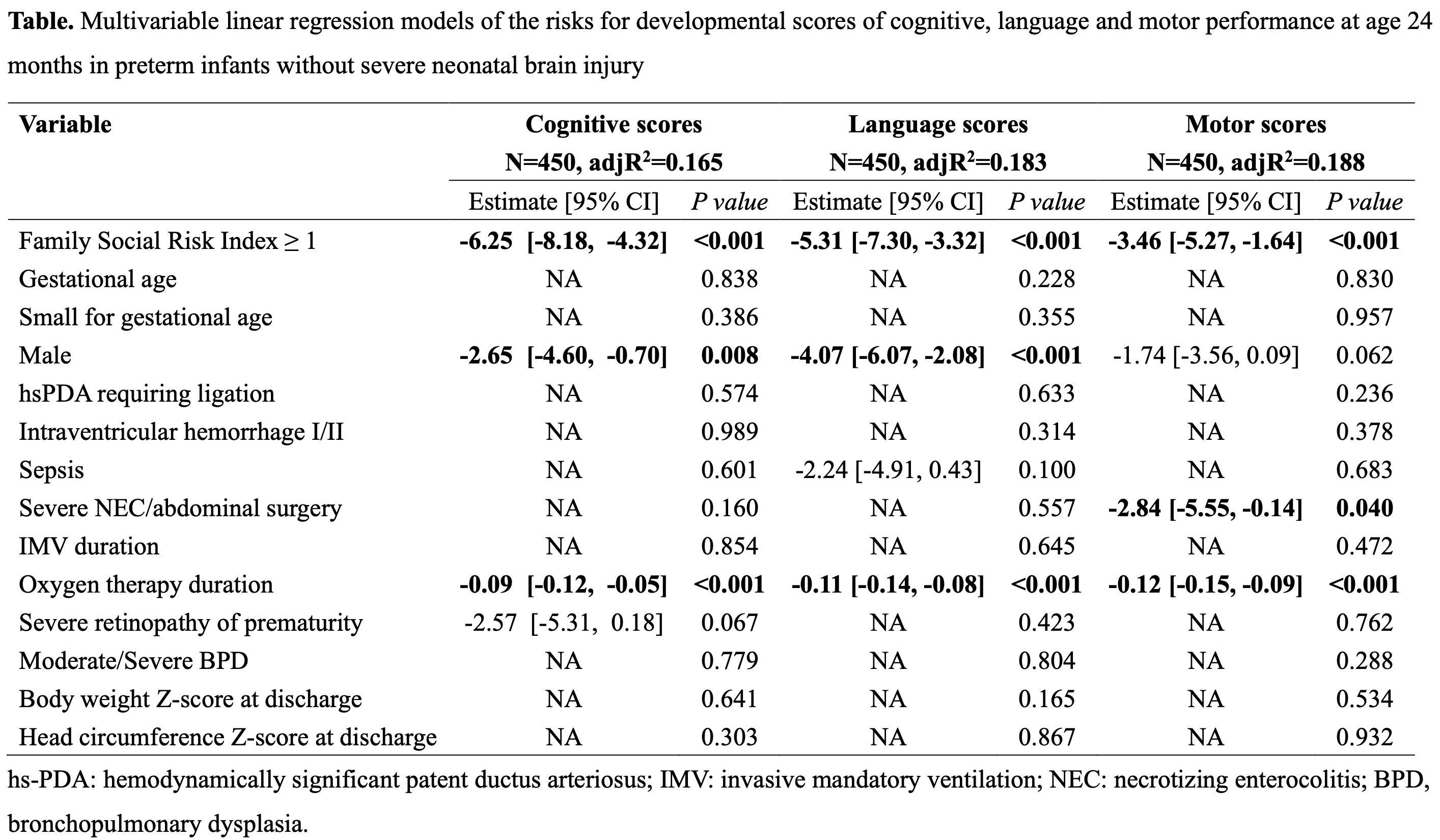 Multivariable linear regression models of the risks for developmental scores of cognitive, language and motor performance at age 24 months in extremely preterm infants without severe neonatal brain injury
Multivariable linear regression models of the risks for developmental scores of cognitive, language and motor performance at age 24 months in extremely preterm infants without severe neonatal brain injury 