
Immunizations/Delivery 1
Session: Immunizations/Delivery 1

David Higgins, MD, MPH
Instructor of Pediatrics
University Of Colorado School Of Medicine
Centennial, Colorado, United States
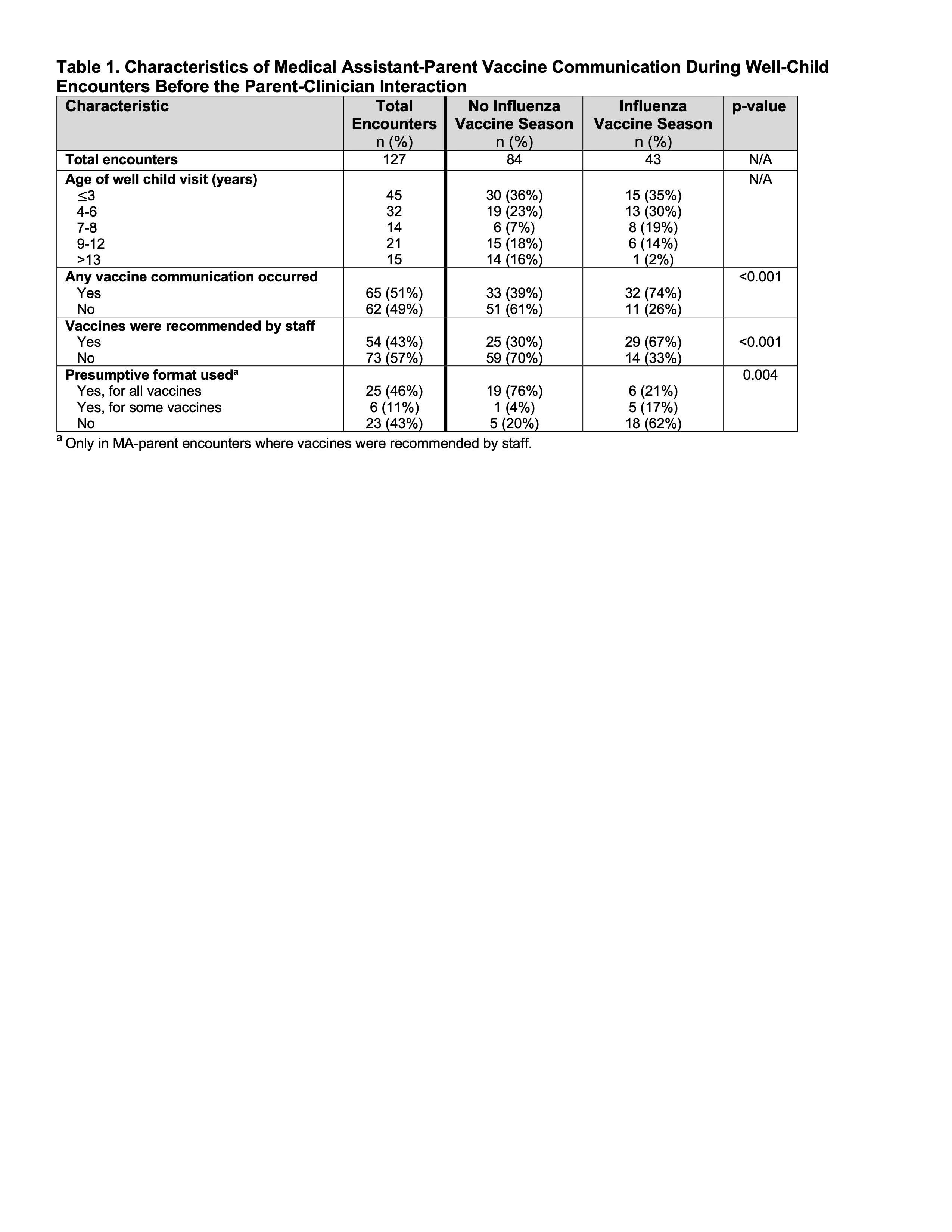 Characteristics of Medical Assistant-Parent Vaccine Communication During Well-Child Encounters Before the Parent-Clinician Interaction
Characteristics of Medical Assistant-Parent Vaccine Communication During Well-Child Encounters Before the Parent-Clinician Interaction.jpg) Key Observations of Medical Assistant-Parent Vaccine Communication During Well-Child Encounters Before the Clinician-Parent Interaction
Key Observations of Medical Assistant-Parent Vaccine Communication During Well-Child Encounters Before the Clinician-Parent Interaction