
Neonatal General 1: Respiratory, BPD
Session: Neonatal General 1: Respiratory, BPD
Ori Hochwald, MD (he/him/his)
Head of NICU
Rambam Medical Center, Haifa, Israel
Haifa, Hefa, Israel
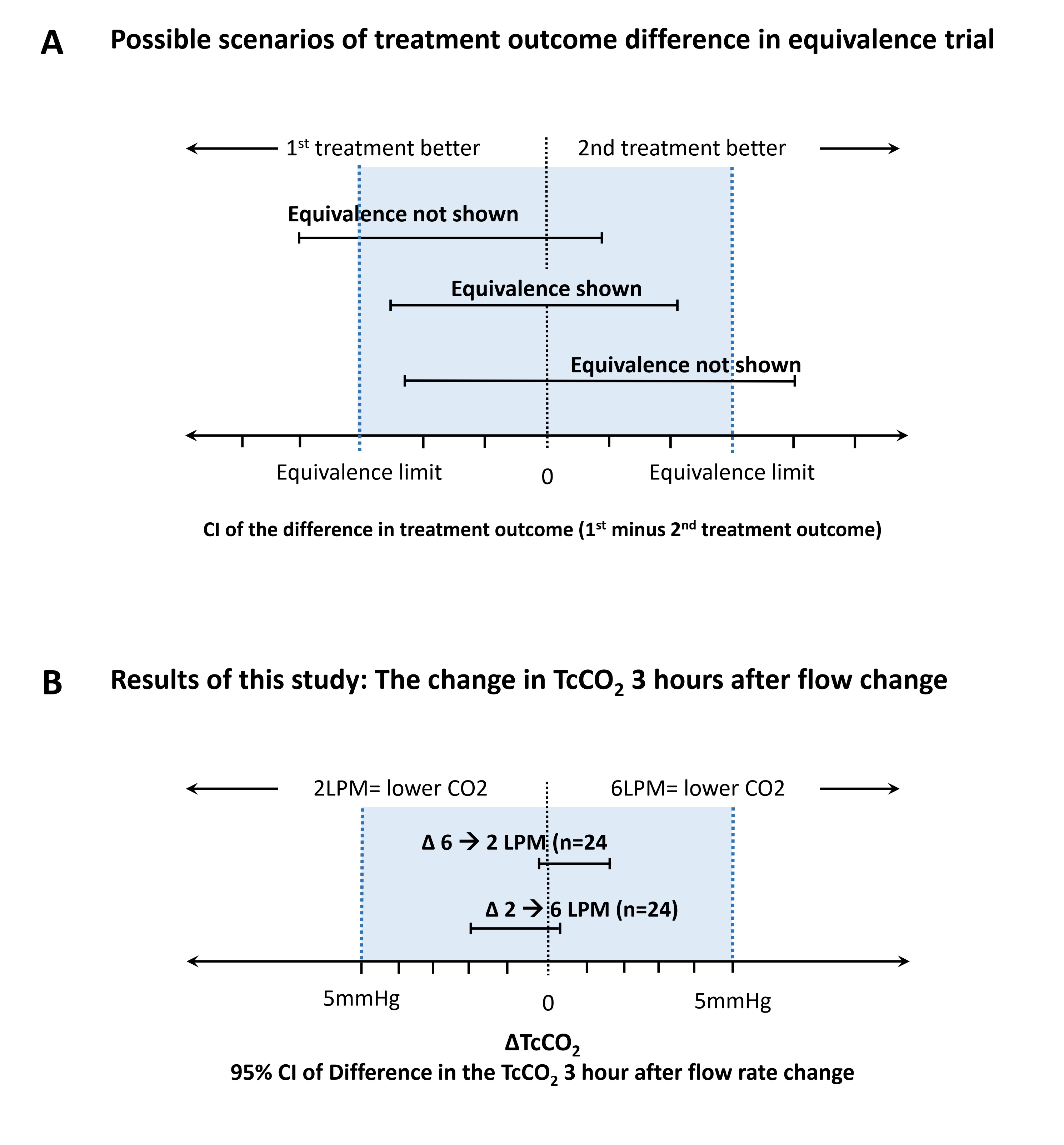 A. Possible scenarios of results for a Equivalence trial according to Piaggio et al. (2012, JAMA)A. Possible scenarios of results for a Equivalence trial according to Piaggio et al. (2012, JAMA)
A. Possible scenarios of results for a Equivalence trial according to Piaggio et al. (2012, JAMA)A. Possible scenarios of results for a Equivalence trial according to Piaggio et al. (2012, JAMA)