
Neonatal/Infant Resuscitation 1
Session: Neonatal/Infant Resuscitation 1
 photo")
Jacqueline Hannan, PhD (she/her/hers)
Human Factors Researcher
University of Michigan
Ann Arbor, Michigan, United States
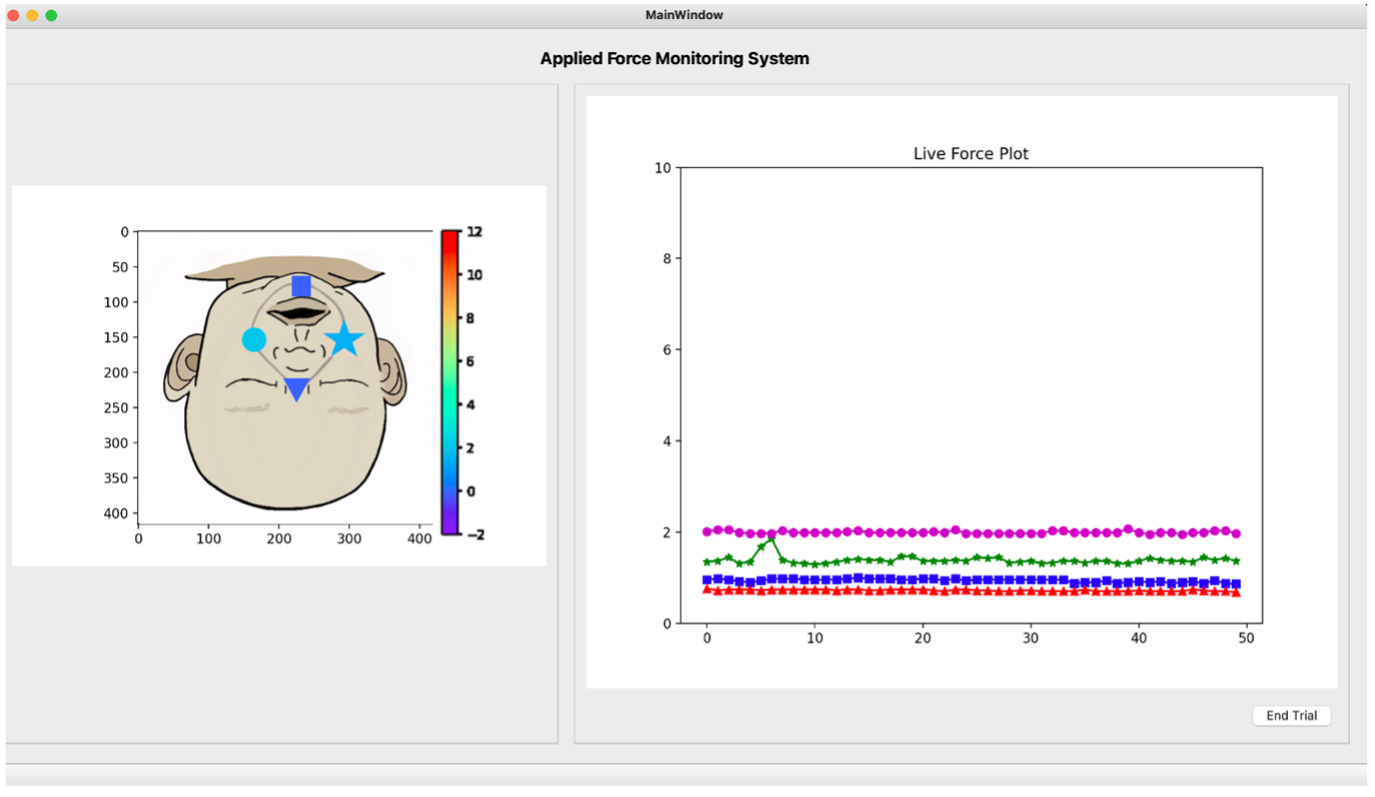 Custom interface designed to present live force feedback; left side: face-mapping diagram, right side: time series plot.
Custom interface designed to present live force feedback; left side: face-mapping diagram, right side: time series plot. 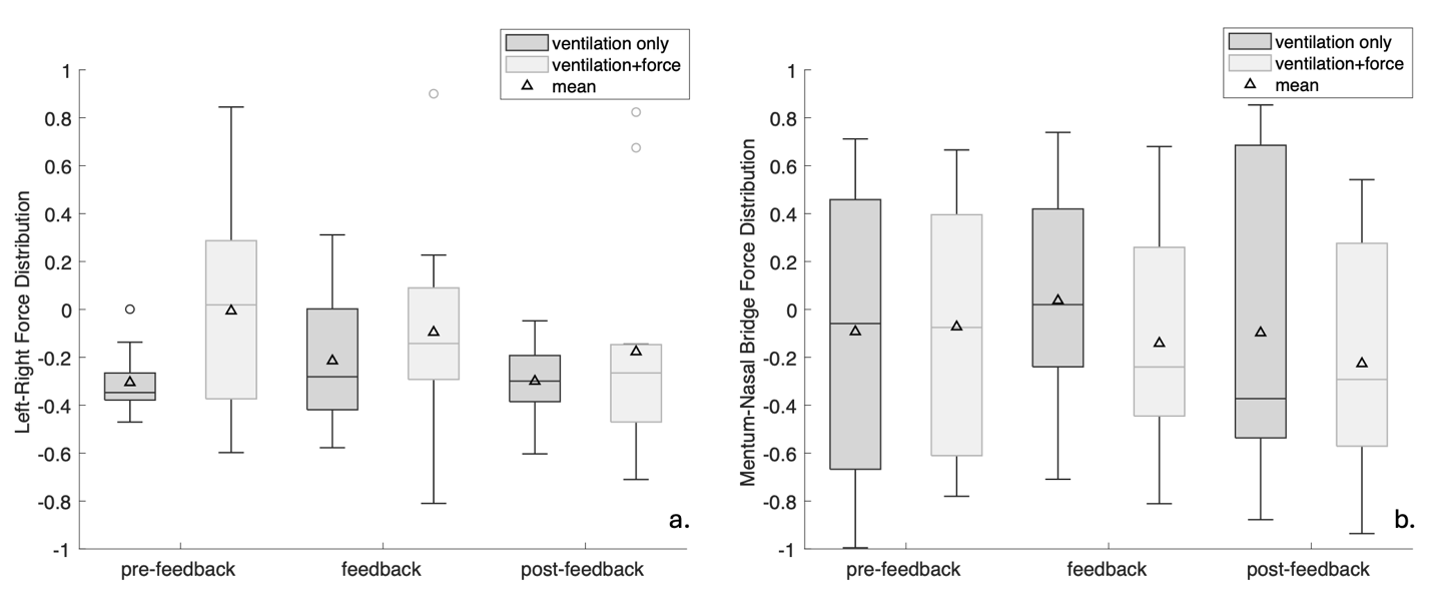 Force distribution on the face sensors for each trial, grouped by feedback condition. Values are represented as a ratio of the force difference to the total force applied in the respective directions. 2a. Average left-right force distribution for each trial. Positive values indicate greater left force; negative values indicate greater right force. 2b. Average chin-nose force distribution for each trial. Positive values indicate greater chin force; negative values indicate greater nose force.
Force distribution on the face sensors for each trial, grouped by feedback condition. Values are represented as a ratio of the force difference to the total force applied in the respective directions. 2a. Average left-right force distribution for each trial. Positive values indicate greater left force; negative values indicate greater right force. 2b. Average chin-nose force distribution for each trial. Positive values indicate greater chin force; negative values indicate greater nose force. 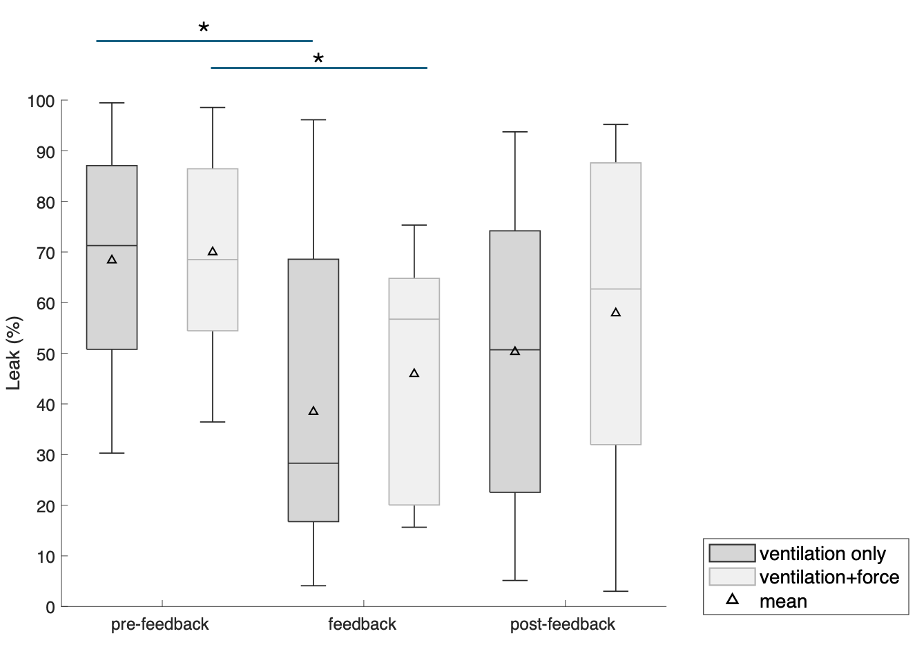 Percent mask leak for each trial, grouped by feedback condition. Asterisk indicates significance between groups. Custom interface designed to present live force feedback; left side: face-mapping diagram, right side: time series plot. Force distribution on the face sensors for each trial, grouped by feedback condition. Values are represented as a ratio of the force difference to the total force applied in the respective directions. 2a. Average left-right force distribution for each trial. Positive values indicate greater left force; negative values indicate greater right force. 2b. Average chin-nose force distribution for each trial. Positive values indicate greater chin force; negative values indicate greater nose force. Percent mask leak for each trial, grouped by feedback condition. Asterisk indicates significance between groups.
Percent mask leak for each trial, grouped by feedback condition. Asterisk indicates significance between groups. Custom interface designed to present live force feedback; left side: face-mapping diagram, right side: time series plot. Force distribution on the face sensors for each trial, grouped by feedback condition. Values are represented as a ratio of the force difference to the total force applied in the respective directions. 2a. Average left-right force distribution for each trial. Positive values indicate greater left force; negative values indicate greater right force. 2b. Average chin-nose force distribution for each trial. Positive values indicate greater chin force; negative values indicate greater nose force. Percent mask leak for each trial, grouped by feedback condition. Asterisk indicates significance between groups. 