
Neonatal Neurology 3
Session: Neonatal Neurology 3
 photo")
Marie Cornet, MD PhD (she/her/hers)
Assistant Professor
UCSF Benioff Children's Hospital San Francisco
San Francisco, California, United States
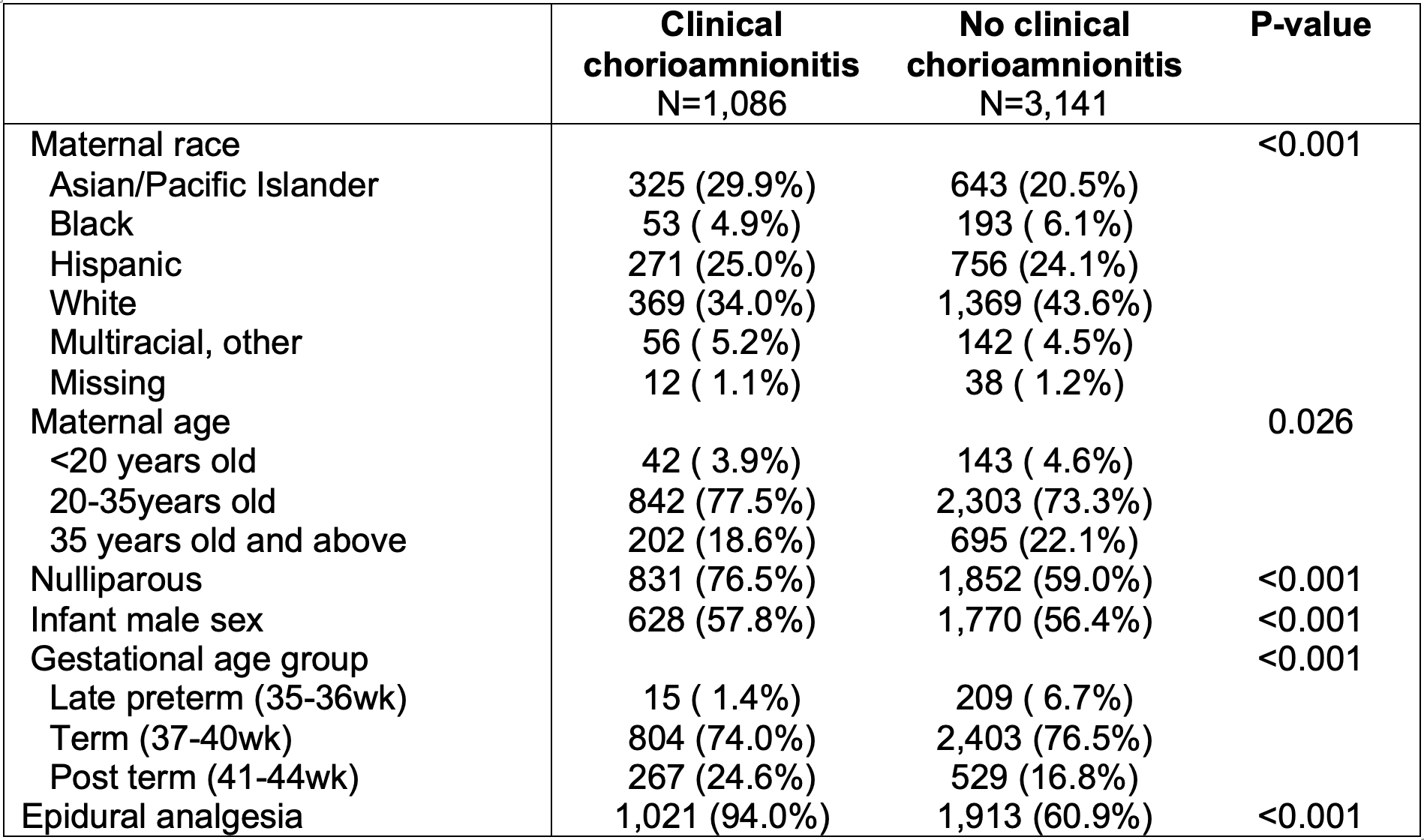
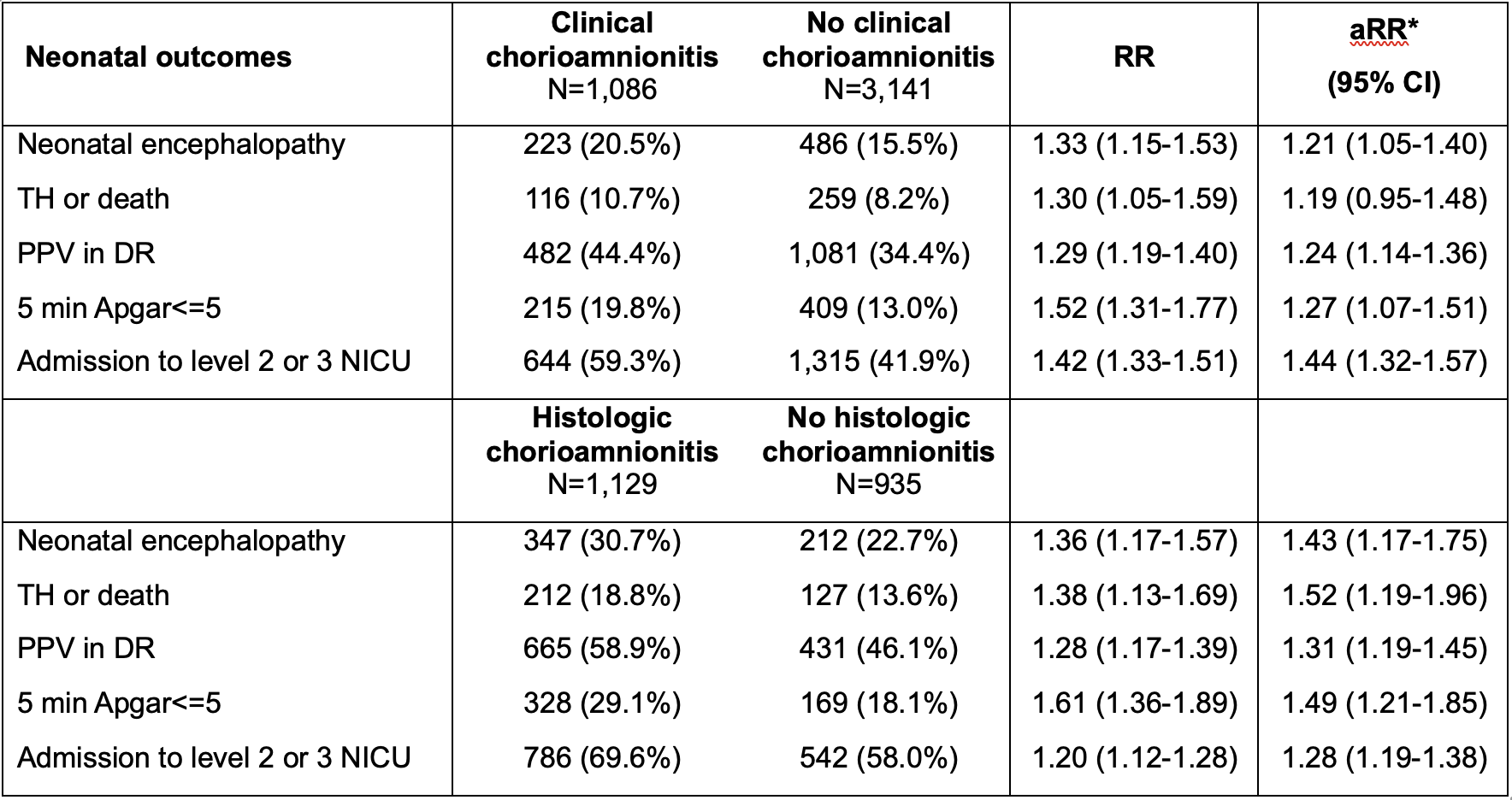 * aRR (adjusted relative risk) calculated by Poisson regression with robust standard error clustered by the hospital and adjusting for all factors included in Table 1: race, maternal age, parity status, infant sex, gestational age, epidural, and degree of acidosis as a spline.
* aRR (adjusted relative risk) calculated by Poisson regression with robust standard error clustered by the hospital and adjusting for all factors included in Table 1: race, maternal age, parity status, infant sex, gestational age, epidural, and degree of acidosis as a spline. 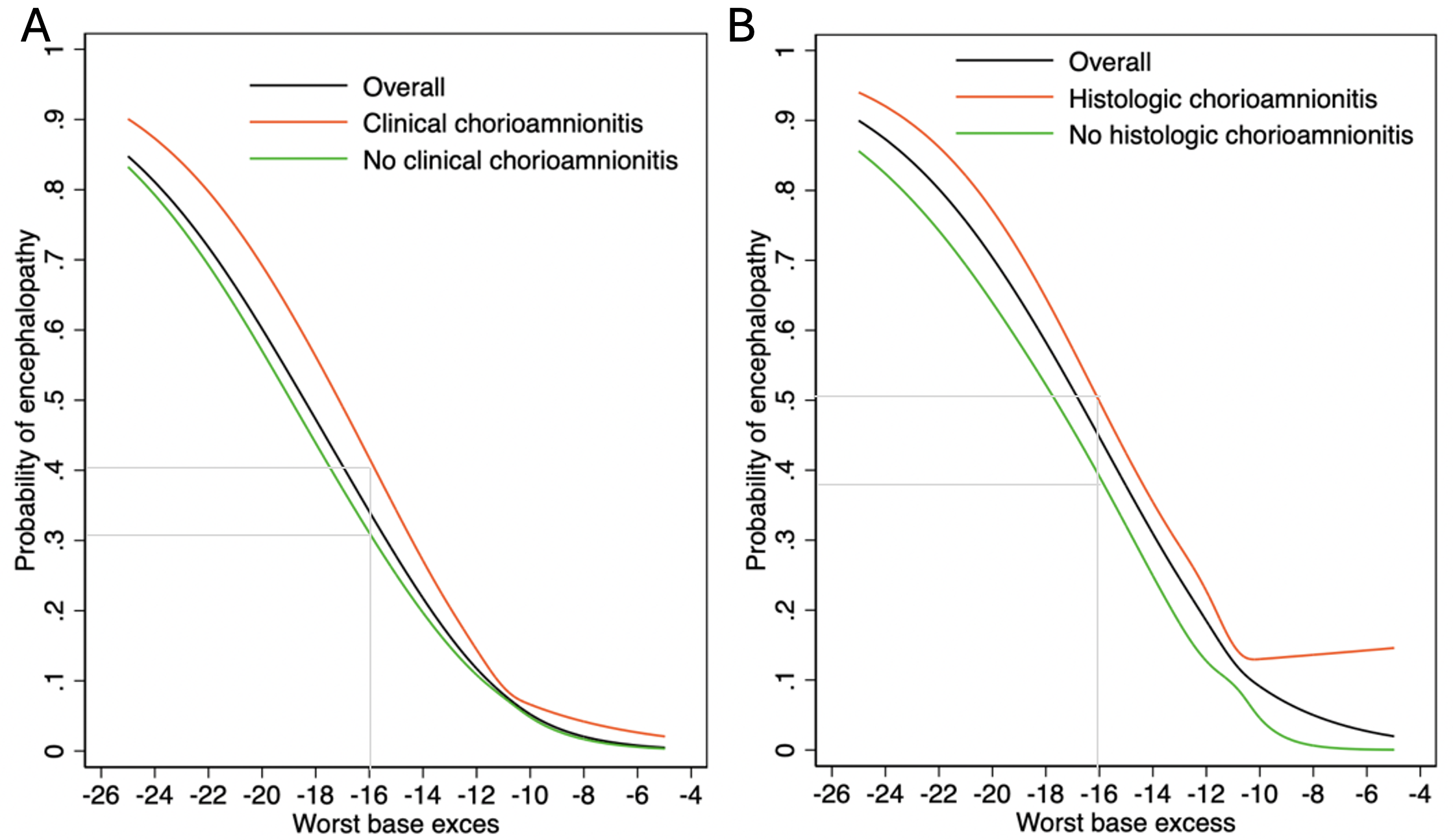 The probability was calculated by constructing a logistic regression model, adjusting for the worst base excess (BE) as a spline. For a worst BE of -16, 42% of infants exposed to clinical chorioamnionitis had encephalopathy compared to 31% of unexposed infants (Risk difference 8.4% [95%CI 4.2-12.6%]). Similarly, among infants with a placenta available, for a worst BE of -16, 51% of infants exposed to histologic chorioamnionitis had encephalopathy compared to 38% of unexposed infants (Risk difference 15.1% [95%CI 9.8-20.4%]). * aRR (adjusted relative risk) calculated by Poisson regression with robust standard error clustered by the hospital and adjusting for all factors included in Table 1: race, maternal age, parity status, infant sex, gestational age, epidural, and degree of acidosis as a spline. The probability was calculated by constructing a logistic regression model, adjusting for the worst base excess (BE) as a spline. For a worst BE of -16, 42% of infants exposed to clinical chorioamnionitis had encephalopathy compared to 31% of unexposed infants (Risk difference 8.4% [95%CI 4.2-12.6%]). Similarly, among infants with a placenta available, for a worst BE of -16, 51% of infants exposed to histologic chorioamnionitis had encephalopathy compared to 38% of unexposed infants (Risk difference 15.1% [95%CI 9.8-20.4%]).
The probability was calculated by constructing a logistic regression model, adjusting for the worst base excess (BE) as a spline. For a worst BE of -16, 42% of infants exposed to clinical chorioamnionitis had encephalopathy compared to 31% of unexposed infants (Risk difference 8.4% [95%CI 4.2-12.6%]). Similarly, among infants with a placenta available, for a worst BE of -16, 51% of infants exposed to histologic chorioamnionitis had encephalopathy compared to 38% of unexposed infants (Risk difference 15.1% [95%CI 9.8-20.4%]). * aRR (adjusted relative risk) calculated by Poisson regression with robust standard error clustered by the hospital and adjusting for all factors included in Table 1: race, maternal age, parity status, infant sex, gestational age, epidural, and degree of acidosis as a spline. The probability was calculated by constructing a logistic regression model, adjusting for the worst base excess (BE) as a spline. For a worst BE of -16, 42% of infants exposed to clinical chorioamnionitis had encephalopathy compared to 31% of unexposed infants (Risk difference 8.4% [95%CI 4.2-12.6%]). Similarly, among infants with a placenta available, for a worst BE of -16, 51% of infants exposed to histologic chorioamnionitis had encephalopathy compared to 38% of unexposed infants (Risk difference 15.1% [95%CI 9.8-20.4%]). 