
Neonatal Hemodynamics and Cardiovascular Medicine 2
Session: Neonatal Hemodynamics and Cardiovascular Medicine 2

Shazia Bhombal, MD
Associate Professor
Children’s Healthcare of Atlanta/Emory University
Atlanta, Georgia, United States
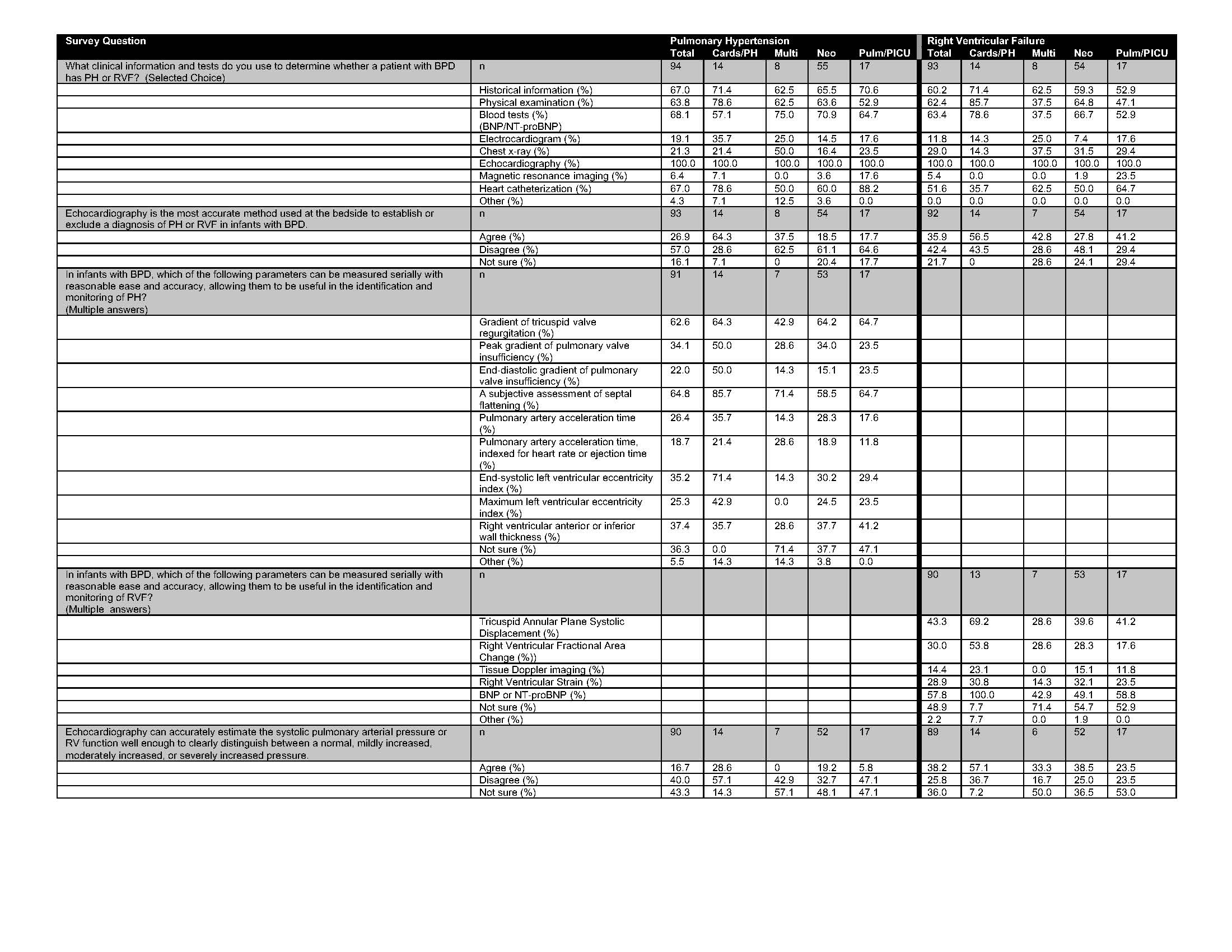 Multiple-choice responses to questions evaluating pulmonary hypertension and right ventricular failure in infants with BPD are shown. The total number of respondents (n) is listed in the top row (gray) and percentage by subspeciality is shown below each question.
Multiple-choice responses to questions evaluating pulmonary hypertension and right ventricular failure in infants with BPD are shown. The total number of respondents (n) is listed in the top row (gray) and percentage by subspeciality is shown below each question.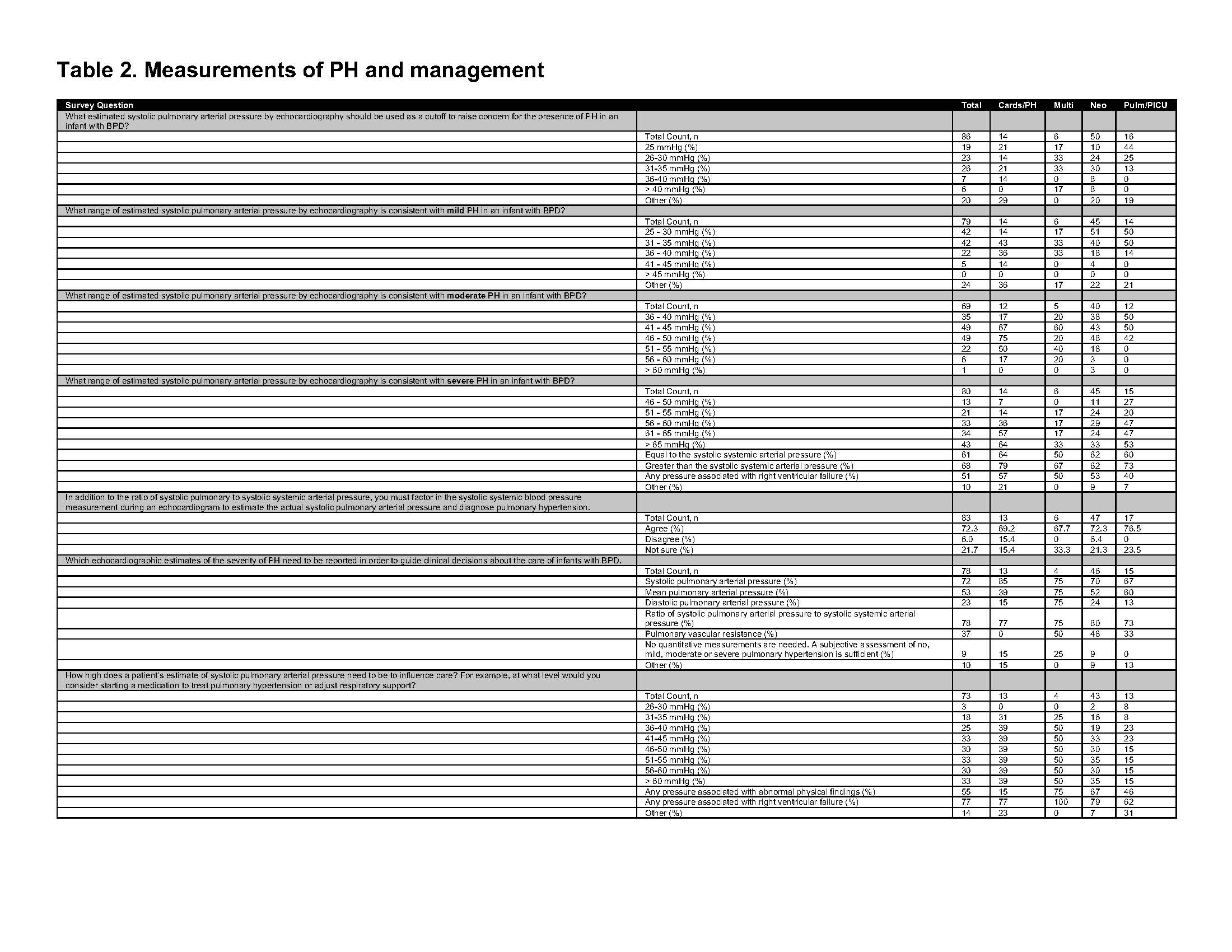 Multiple-choice responses for questions evaluating thresholds for echocardiographic parameters for the diagnosis and treatment of PH and RVF are shown. The total number of respondents (n) are shown in the top row (in gray), and the percentage of respondents by sub-specialty are shown below each question.
Multiple-choice responses for questions evaluating thresholds for echocardiographic parameters for the diagnosis and treatment of PH and RVF are shown. The total number of respondents (n) are shown in the top row (in gray), and the percentage of respondents by sub-specialty are shown below each question.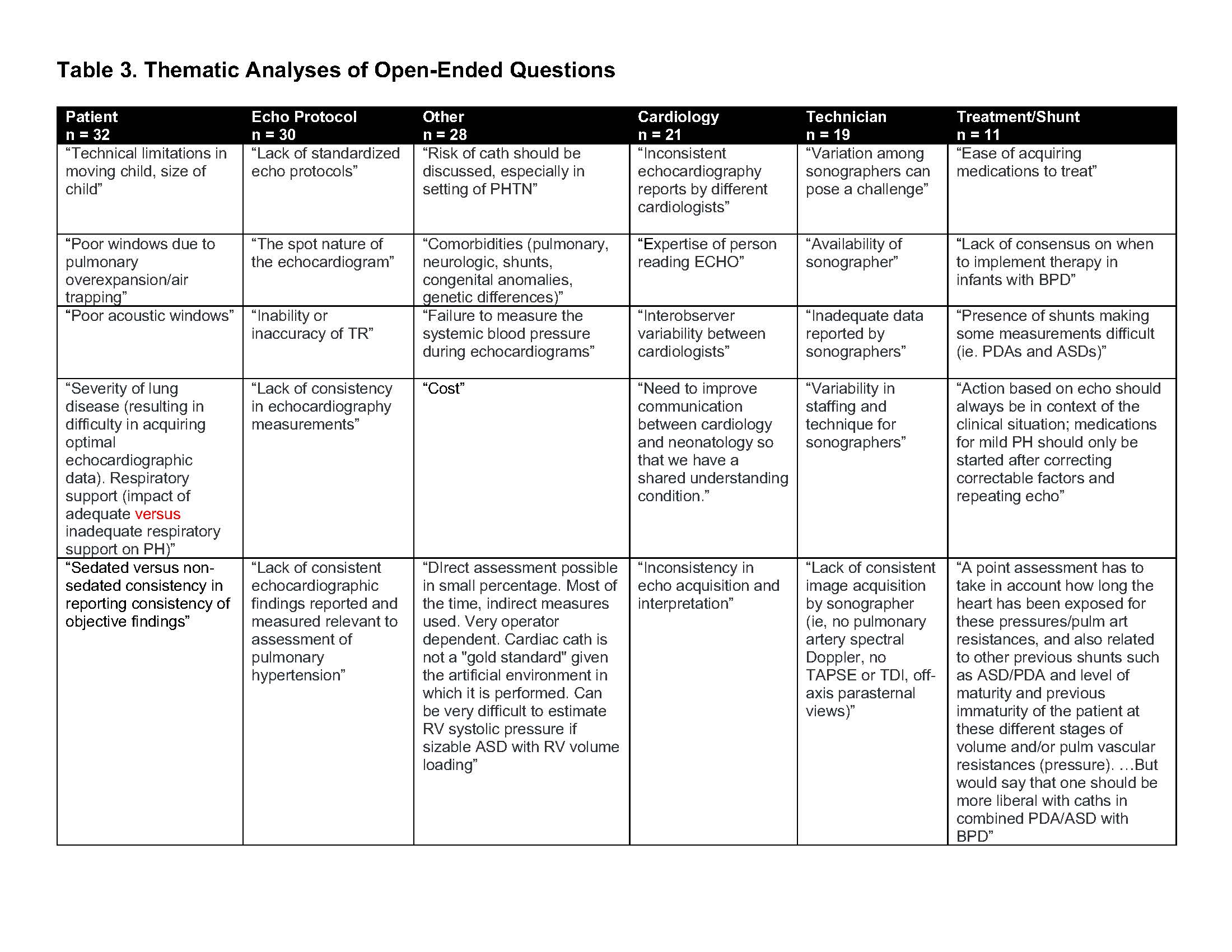 Shown are representative quotations for the six major themes identified through open-ended questions. The total number of responses per theme is indicated in the black heading (n).
Shown are representative quotations for the six major themes identified through open-ended questions. The total number of responses per theme is indicated in the black heading (n).