
Neonatal Hemodynamics and Cardiovascular Medicine 2
Session: Neonatal Hemodynamics and Cardiovascular Medicine 2

Shazia Bhombal, MD
Associate Professor
Children’s Healthcare of Atlanta/Emory University
Atlanta, Georgia, United States
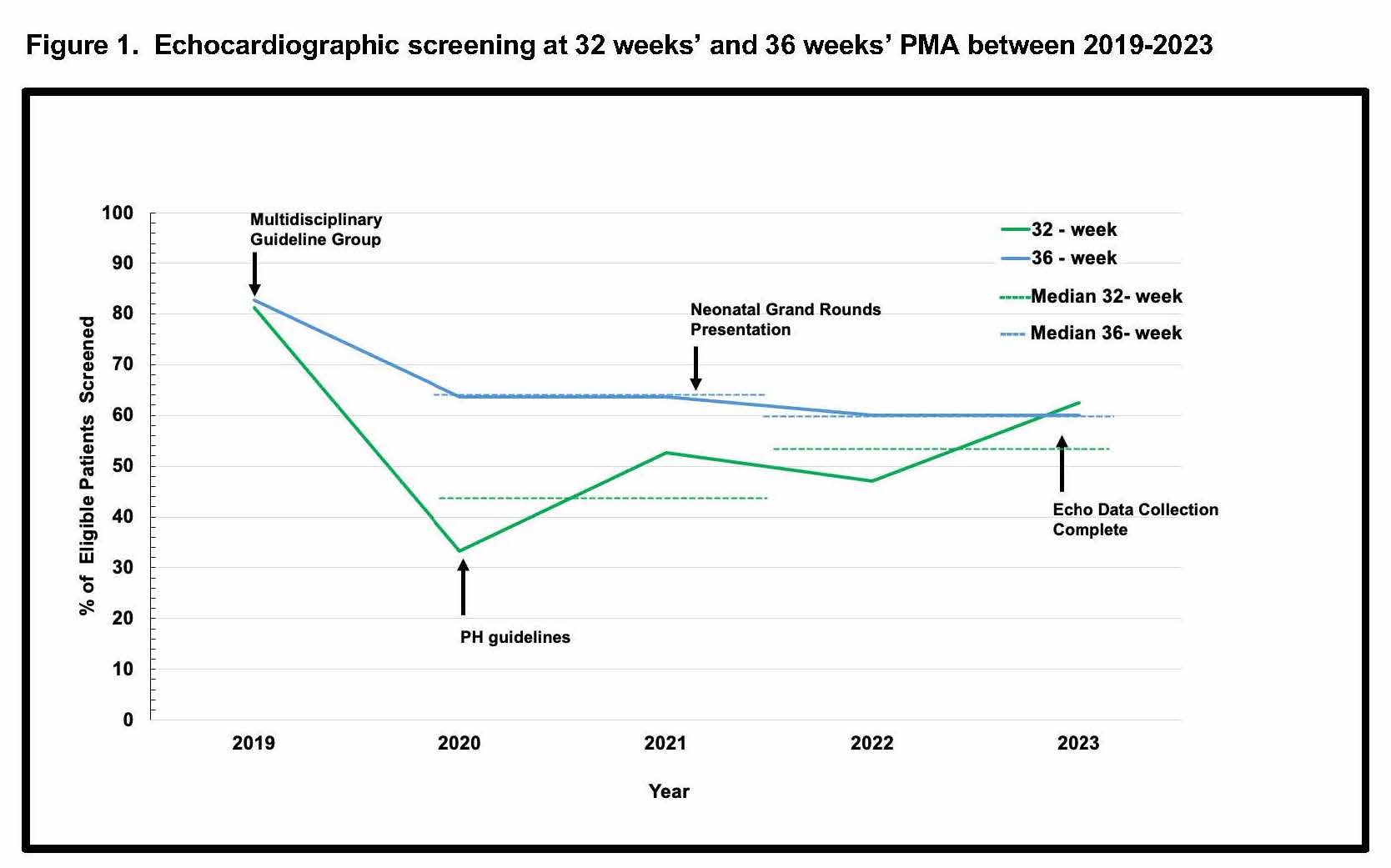 The percentage of echocardiographs performed at 32 weeks' PMA (green) and 36 weeks' PMA (blue), along with median values (dashed lines) are shown by year over the study period.
The percentage of echocardiographs performed at 32 weeks' PMA (green) and 36 weeks' PMA (blue), along with median values (dashed lines) are shown by year over the study period. .jpg) Demographic characteristics and selected echocardiographic parameters at 36 weeks' are shown. Abbreviations: LPM -- liters per minute; IMV -- Invasive mechanical ventilation; HFOV - high-frequency oscillatory ventilation; PFO -- patent foramen ovale; ASD -- atrial septal defect. Statistical tests used are shown at the bottom of the table, * p < 0.05 was significant.
Demographic characteristics and selected echocardiographic parameters at 36 weeks' are shown. Abbreviations: LPM -- liters per minute; IMV -- Invasive mechanical ventilation; HFOV - high-frequency oscillatory ventilation; PFO -- patent foramen ovale; ASD -- atrial septal defect. Statistical tests used are shown at the bottom of the table, * p < 0.05 was significant..jpg) Stepwise AIC, LASSO regression, and Random Forest models were applied to identify the most important predictors of PH at discharge. Shown are odds ratios, 95% confidence intervals. PFO -- patent foramen ovale; ASD -- atrial septal defect. *p < 0.05.
Stepwise AIC, LASSO regression, and Random Forest models were applied to identify the most important predictors of PH at discharge. Shown are odds ratios, 95% confidence intervals. PFO -- patent foramen ovale; ASD -- atrial septal defect. *p < 0.05.