Hospital Medicine 1: Quality Improvement
Session: Hospital Medicine 1: Quality Improvement
 Credit")
Ann Kennon Ulicny, DO (she/her/hers)
Pediatric Hospital Medicine Fellow
UAB Pediatrics/Children's of Alabama
Birmingham, Alabama, United States
.png) This p-Chart shows a mean shift from 52% to 66.3% (a 27.5% increase) in the percentage of change in clinical status events with a documented patient update note.
This p-Chart shows a mean shift from 52% to 66.3% (a 27.5% increase) in the percentage of change in clinical status events with a documented patient update note. .png) This key driver diagram highlights that competing priorities, lack of clear guidelines surrounding documentation expectations, perception that verbal handoff is adequate and fear of adding to tension between providers are key barriers to documentation of patient update notes. By eliciting this information through brainstorming sessions, the team was able to develop targeted interventions to reach our SMART aim.
This key driver diagram highlights that competing priorities, lack of clear guidelines surrounding documentation expectations, perception that verbal handoff is adequate and fear of adding to tension between providers are key barriers to documentation of patient update notes. By eliciting this information through brainstorming sessions, the team was able to develop targeted interventions to reach our SMART aim. 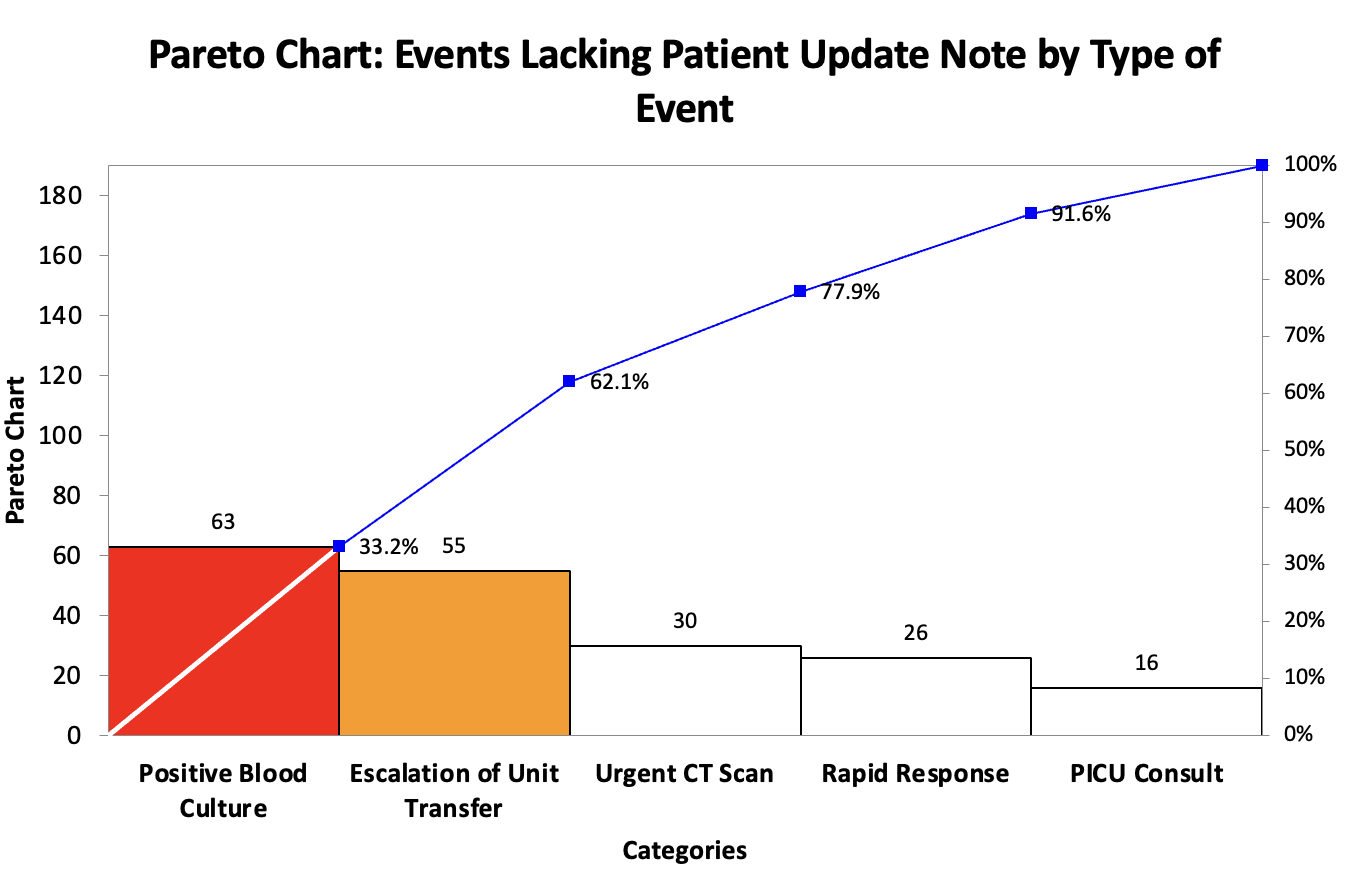 This pareto chart reveals that the most frequent events lacking a patient update note are the occurrence of a positive blood culture and an escalation of unit transfer.
This pareto chart reveals that the most frequent events lacking a patient update note are the occurrence of a positive blood culture and an escalation of unit transfer.