
Quality Improvement/Patient Safety 6
Session: Quality Improvement/Patient Safety 6
 Credit")
 photo")
Melissa Blumberg, MD (she/her/hers)
Fellow
Nemours Children's Hospital
Audubon, New Jersey, United States
.png) The key driver diagram depicts drivers and change ideas affecting our primary aim.
The key driver diagram depicts drivers and change ideas affecting our primary aim. 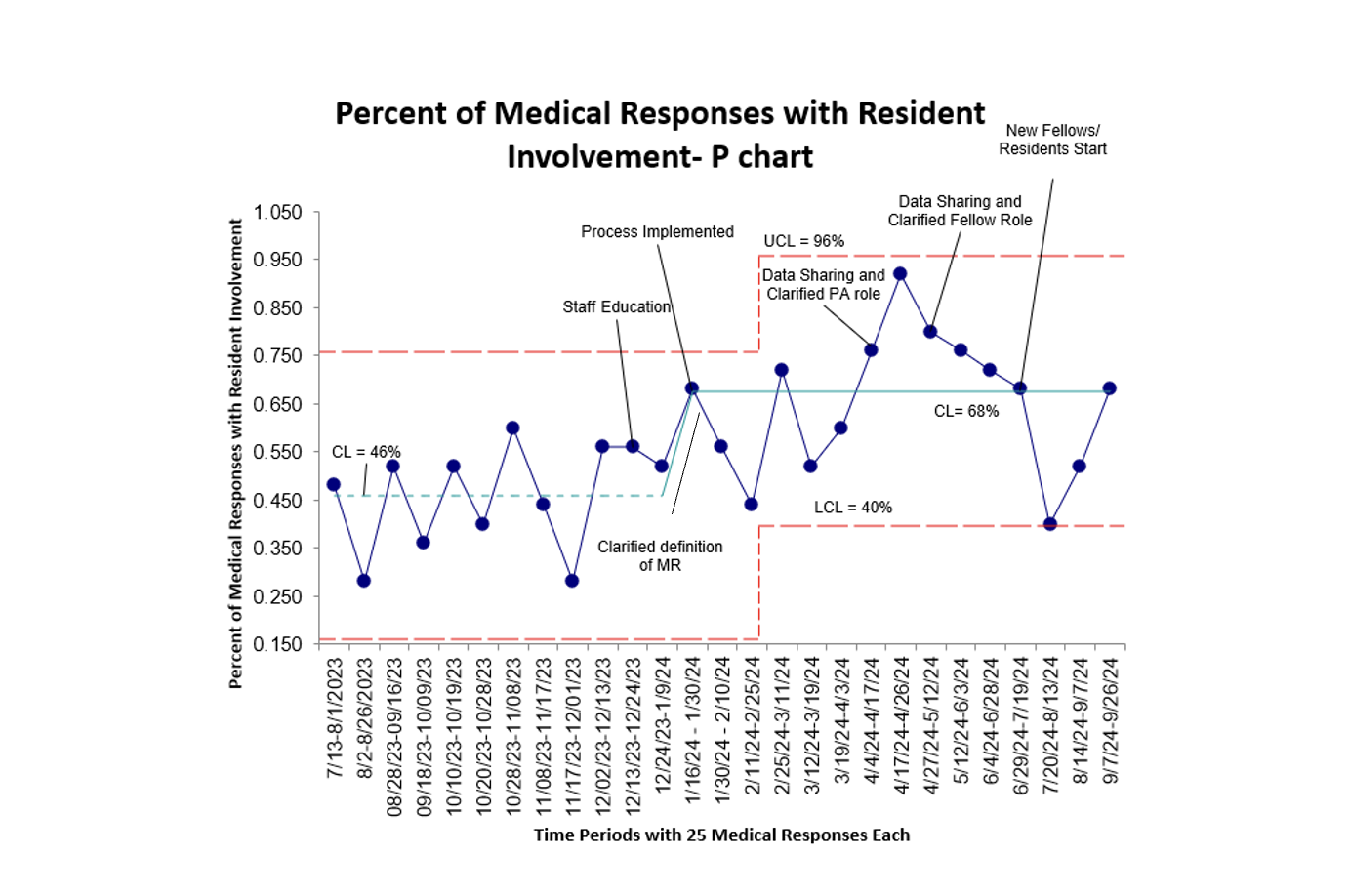 This chart depicts the percent of medical responses with resident involvement over time. Each time period represents 25 individual medical responses.
This chart depicts the percent of medical responses with resident involvement over time. Each time period represents 25 individual medical responses.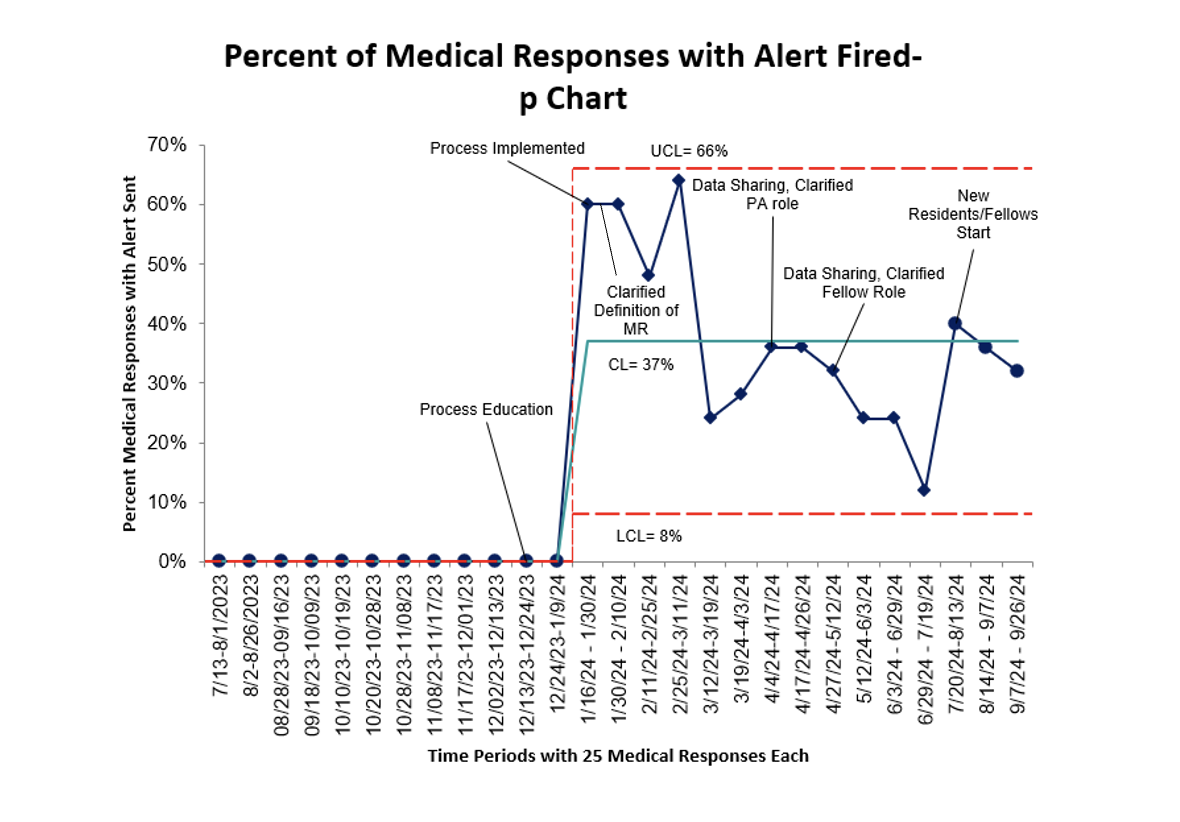 This chart depicts the percent of medical responses with an alert fired over time. Each time period represents 25 individual medical responses.
This chart depicts the percent of medical responses with an alert fired over time. Each time period represents 25 individual medical responses.