
Neonatal Quality Improvement 4
Session: Neonatal Quality Improvement 4
 Credit")
 photo")
Andrew M. Barr, MD, MSE (he/him/his)
Clinical Fellow: Neonatal-Perinatal Medicine
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
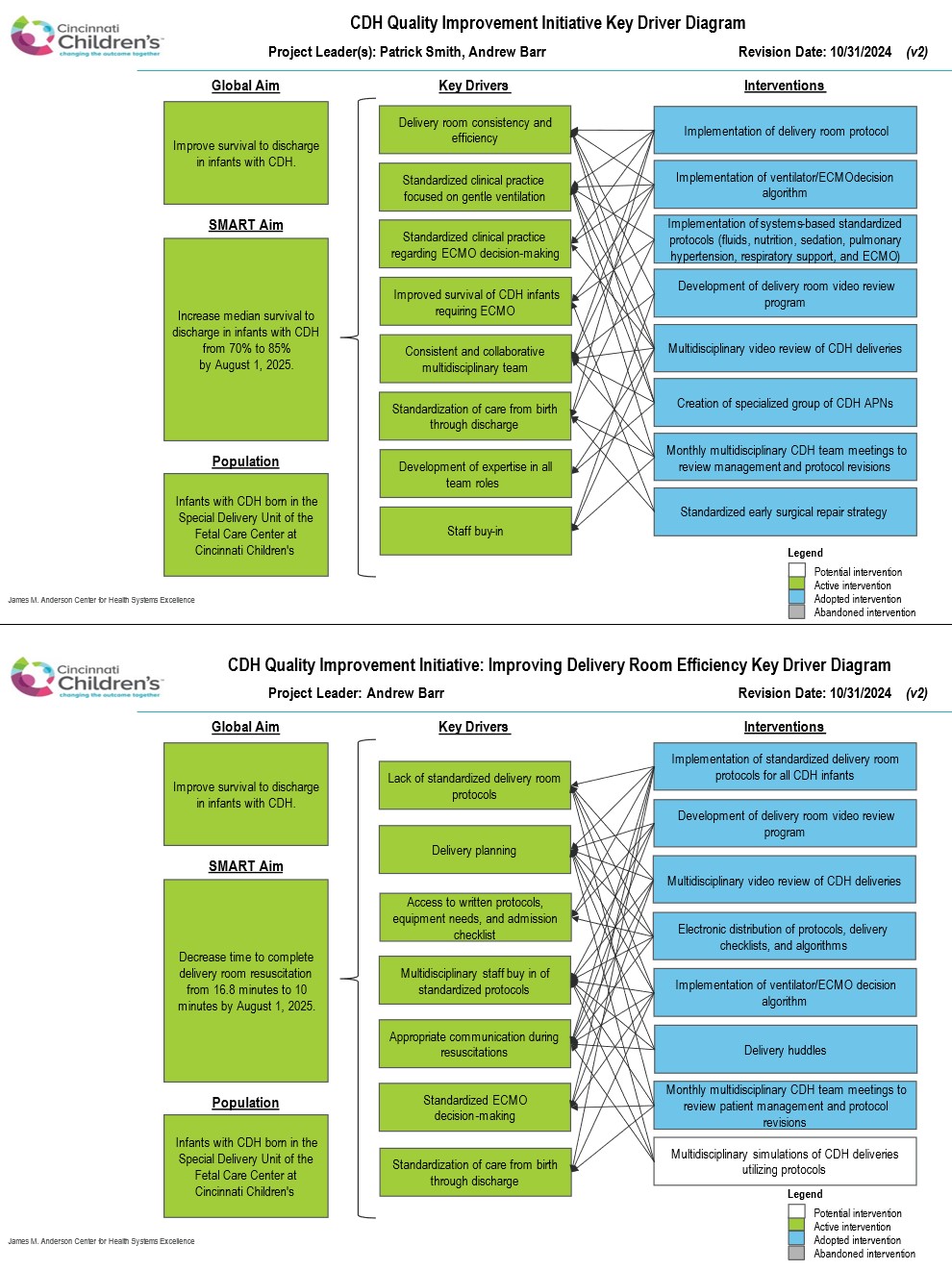 Key driver diagram for the global quality improvement initiative aimed at improving CDH survival (top) and the key driver diagram for improving delivery room consistency and efficiency (bottom), a key driver of our global aim.
Key driver diagram for the global quality improvement initiative aimed at improving CDH survival (top) and the key driver diagram for improving delivery room consistency and efficiency (bottom), a key driver of our global aim.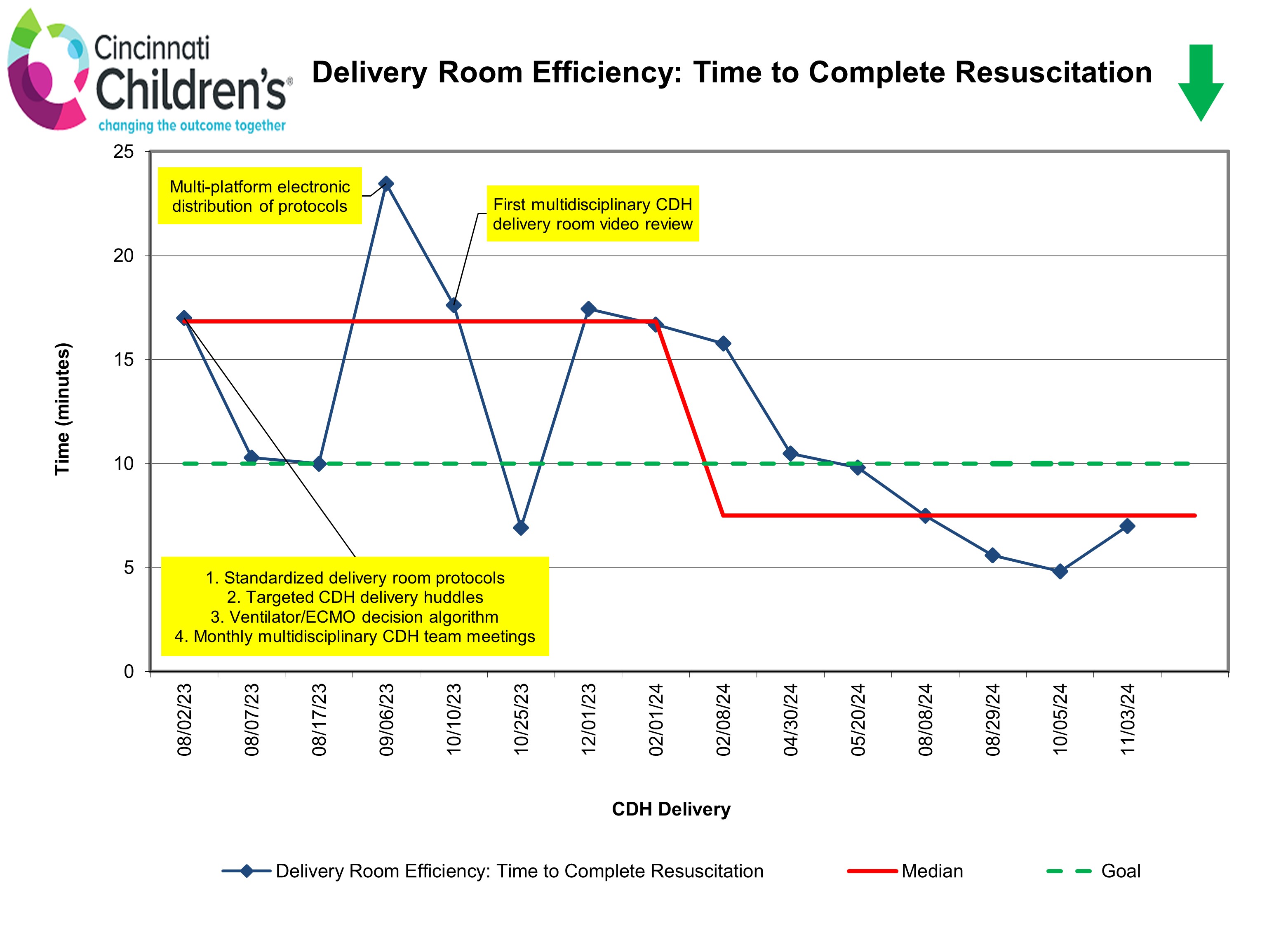 Run chart for time to complete delivery room resuscitation for CDH infants utilizing standardized protocols, defined as the time from arrival to infant warmer bed to completion of the final step of the protocol (IV access), assessed as a process measure marking efficiency. After implementation of standardized protocols and additional interventions as noted, median time to complete resuscitation decreased from a baseline of 16.8 minutes by 55.5% to 7.5 minutes.
Run chart for time to complete delivery room resuscitation for CDH infants utilizing standardized protocols, defined as the time from arrival to infant warmer bed to completion of the final step of the protocol (IV access), assessed as a process measure marking efficiency. After implementation of standardized protocols and additional interventions as noted, median time to complete resuscitation decreased from a baseline of 16.8 minutes by 55.5% to 7.5 minutes.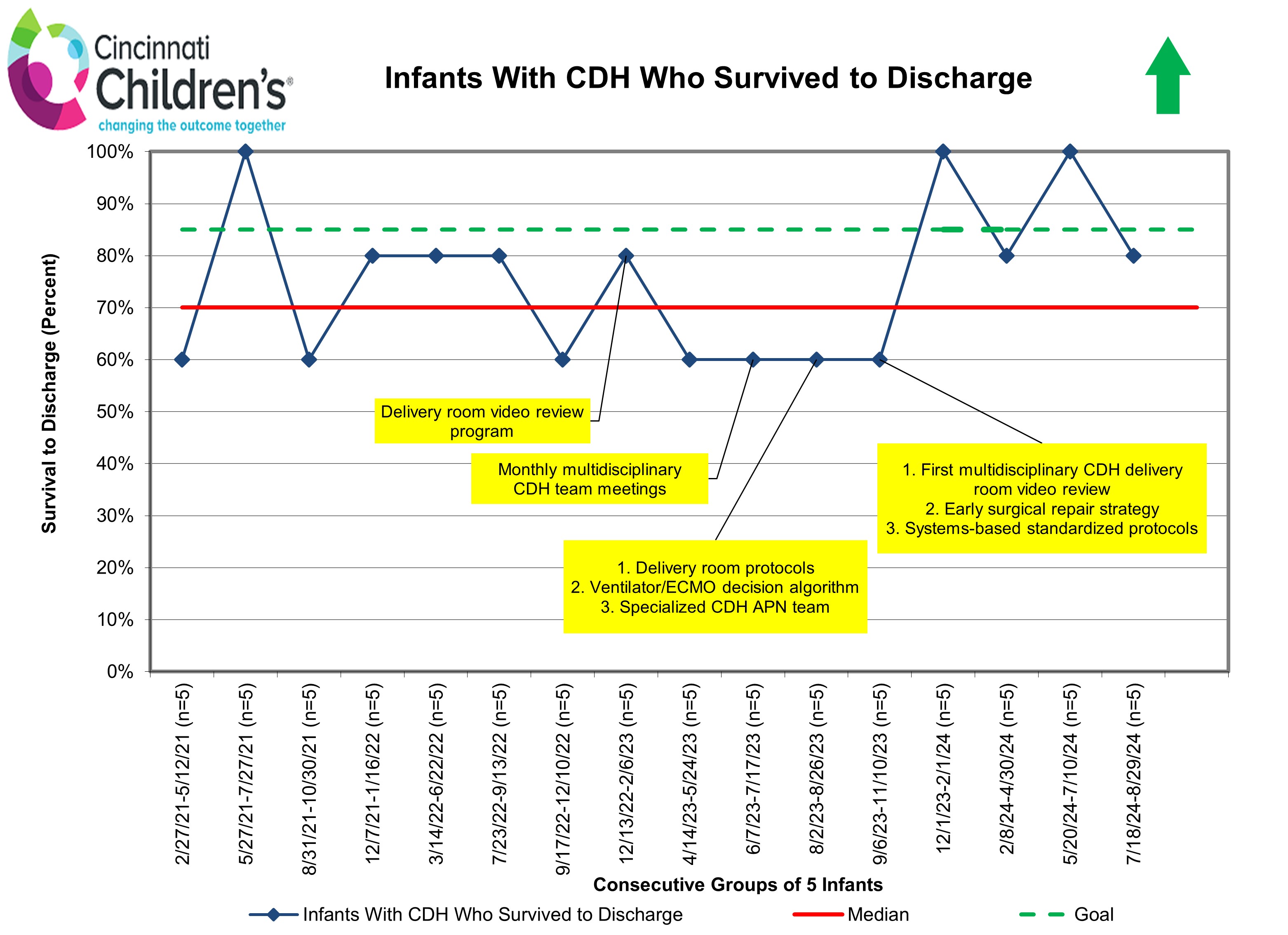 Run chart for survival to discharge of infants with CDH organized in consecutive groups of 5 infants. This shows promising initial improvement in survival to discharge through our QI initiative, and we are hopeful to achieve our global aim of increasing median survival from 70% to 85% by August 2025.
Run chart for survival to discharge of infants with CDH organized in consecutive groups of 5 infants. This shows promising initial improvement in survival to discharge through our QI initiative, and we are hopeful to achieve our global aim of increasing median survival from 70% to 85% by August 2025.