
Neonatal Quality Improvement 4
Session: Neonatal Quality Improvement 4
 Credit")

Oludare A. A. Odumade, MD PhD
Assistant Professor
University of Minnesota Medical School
Minneapolis, Minnesota, United States
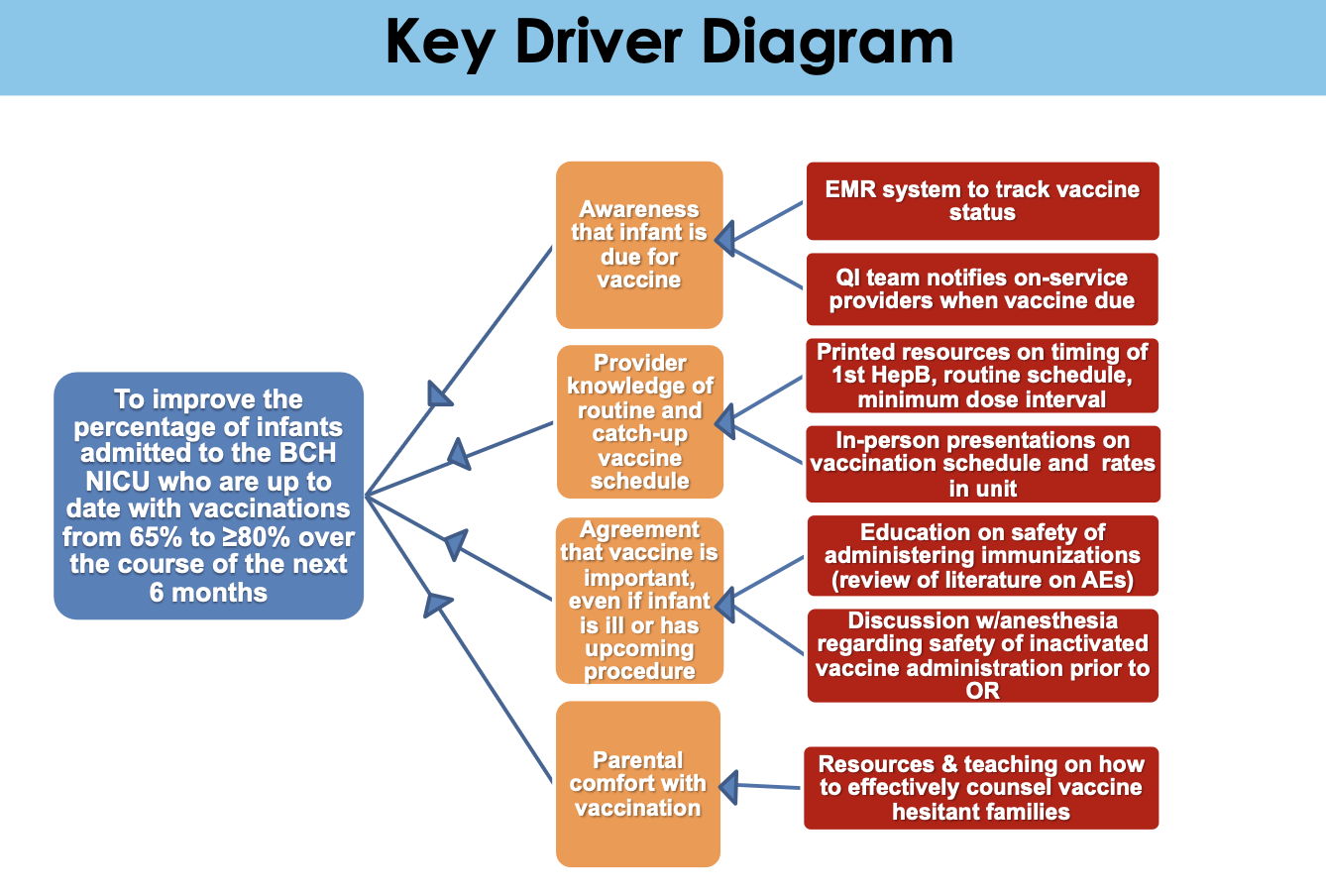 Abbreviations: AE-adverse events, BCH-Boston Children’s Hospital, EMR-electronic medical records, HepB- Hepatitis B vaccine, OR- operating room, QI-quality improvement.
Abbreviations: AE-adverse events, BCH-Boston Children’s Hospital, EMR-electronic medical records, HepB- Hepatitis B vaccine, OR- operating room, QI-quality improvement.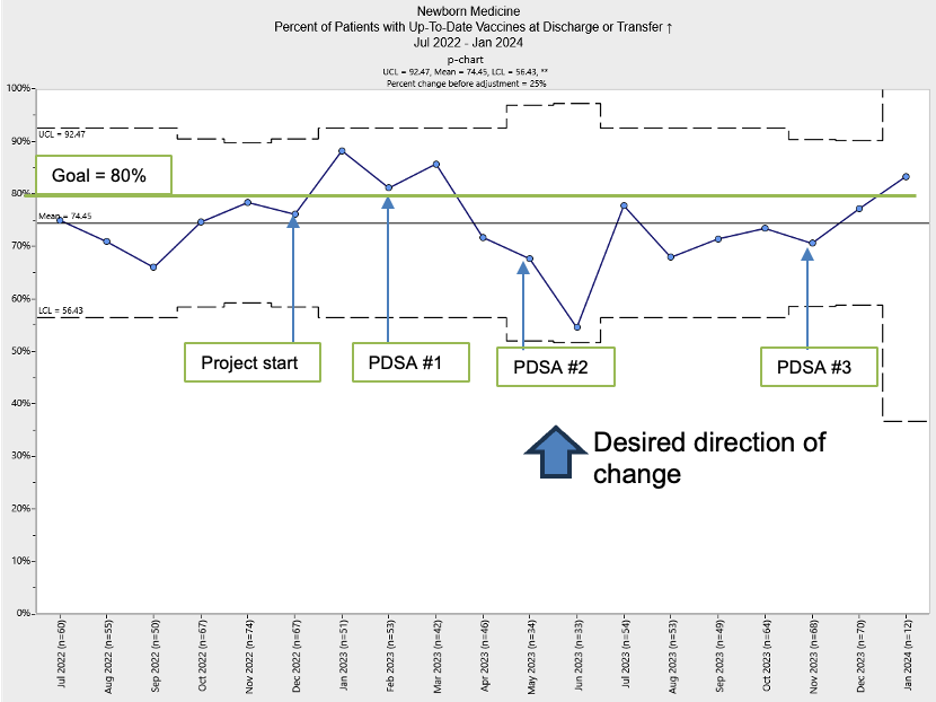 Percent of infants who were up-to-date (UTD) on vaccines at time of discharge/transfer from the Boston Children’s Hospital NICU during the study period (July 2022 to Jan 2024). PDSA cycles depicted in green, monthly rate in blue with goal line at 80% (in green). PDSA Phases: (1) reviewing vaccination status on medical rounds once a week, (2) increasing visibility and awareness with routine healthcare maintenance requirements by placing tracking stickers on the rounding folders, and (3) weekly pharmacy audit and email to increased awareness of vaccination rates prior to discharge within the NICU.
Percent of infants who were up-to-date (UTD) on vaccines at time of discharge/transfer from the Boston Children’s Hospital NICU during the study period (July 2022 to Jan 2024). PDSA cycles depicted in green, monthly rate in blue with goal line at 80% (in green). PDSA Phases: (1) reviewing vaccination status on medical rounds once a week, (2) increasing visibility and awareness with routine healthcare maintenance requirements by placing tracking stickers on the rounding folders, and (3) weekly pharmacy audit and email to increased awareness of vaccination rates prior to discharge within the NICU. 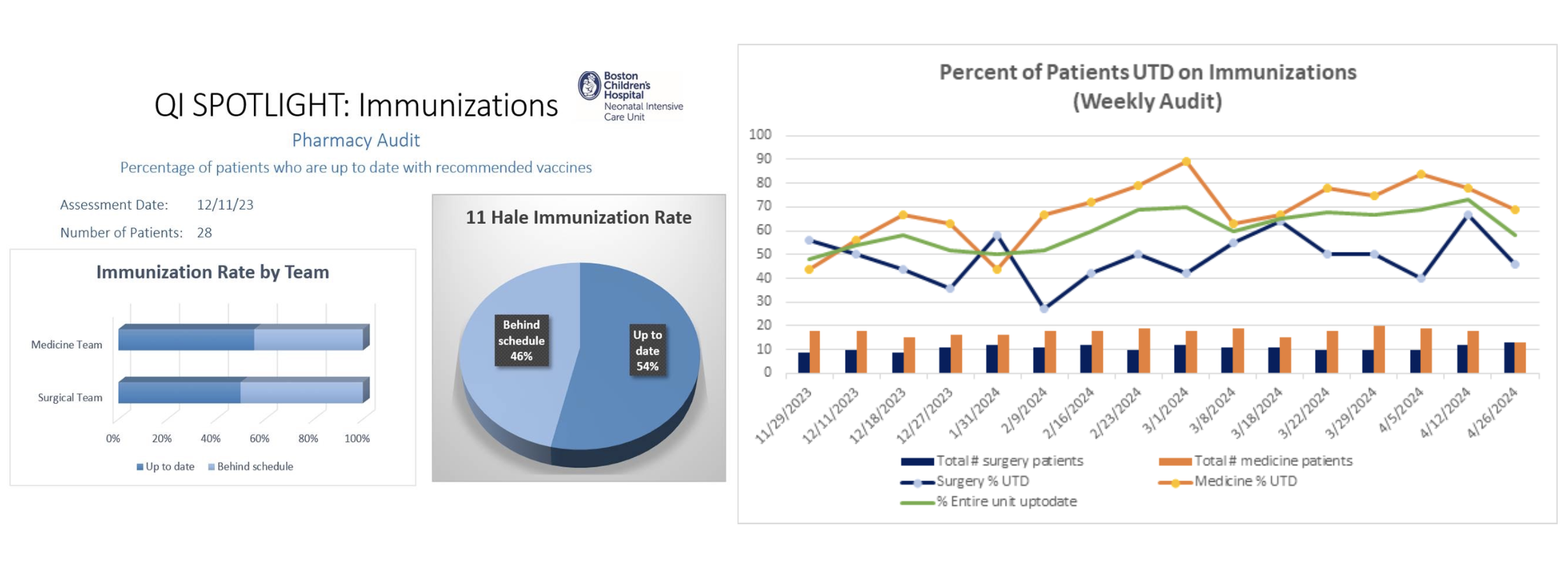 Sample QI spotlight email notification containing rates of up-to-date (UTD) vaccination of infants admitted to Boston Children’s Hospital NICU (left panel) and a longitudinal graph showing differences between the medical and surgical patients (right panel).
Sample QI spotlight email notification containing rates of up-to-date (UTD) vaccination of infants admitted to Boston Children’s Hospital NICU (left panel) and a longitudinal graph showing differences between the medical and surgical patients (right panel).