
Mental Health 1
Session: Mental Health 1
 photo")
Karen C. Manotas, MD (she/her/hers)
Assistant Professor, Department of Psychiatry, Department of Pediatrics
University of Utah Health
Salt Lake City, Utah, United States
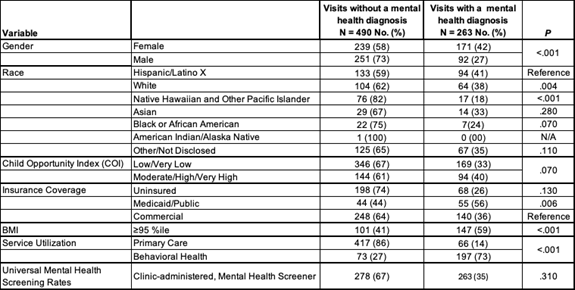 Table 1 Legend. Mental Health Screeners included Pediatric Symptom Checklist- Youth (35 item), Patient Health Questionnaire for Adolescents, and Generalized Anxiety Disorder 7-item.
Table 1 Legend. Mental Health Screeners included Pediatric Symptom Checklist- Youth (35 item), Patient Health Questionnaire for Adolescents, and Generalized Anxiety Disorder 7-item.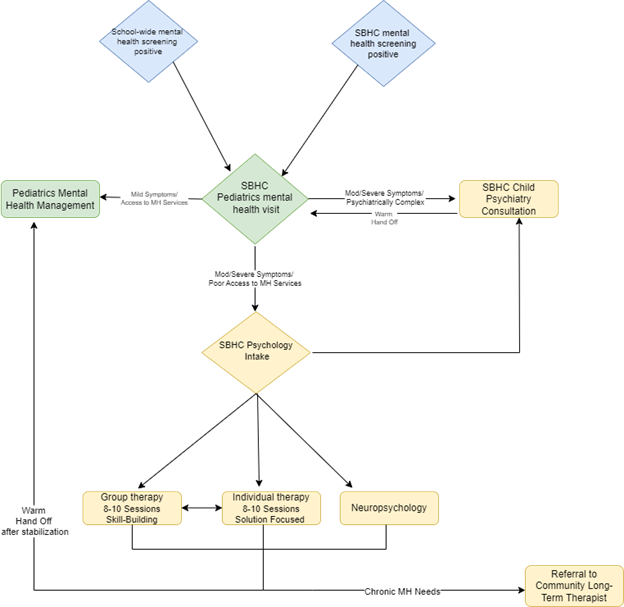 Figure 1 Legend. Blue Diamonds: Tier 1 universal mental health screening as clinic referral sources to School-Based Health Center pediatricians for mental health screening visit.
Figure 1 Legend. Blue Diamonds: Tier 1 universal mental health screening as clinic referral sources to School-Based Health Center pediatricians for mental health screening visit.