
Quality Improvement/Patient Safety 5
Session: Quality Improvement/Patient Safety 5
 photo")
Elizabeth F. Ebbens, MD (she/her/hers)
Pediatric Emergency Medicine Fellow
Monroe Carell Jr. Children's Hospital at Vanderbilt
Madison, Tennessee, United States
.png) Primary measure was percentage of protected notes for adolescents with a positive suicide screen (Columbia--Suicide Severity Rating Scale). Protected notes included both whole protected notes and separate protected confidential notes. Interventions are annotated. Red dots demarcate notable special cause variation associated with embedding confidential note access in the primary ED note.
Primary measure was percentage of protected notes for adolescents with a positive suicide screen (Columbia--Suicide Severity Rating Scale). Protected notes included both whole protected notes and separate protected confidential notes. Interventions are annotated. Red dots demarcate notable special cause variation associated with embedding confidential note access in the primary ED note. 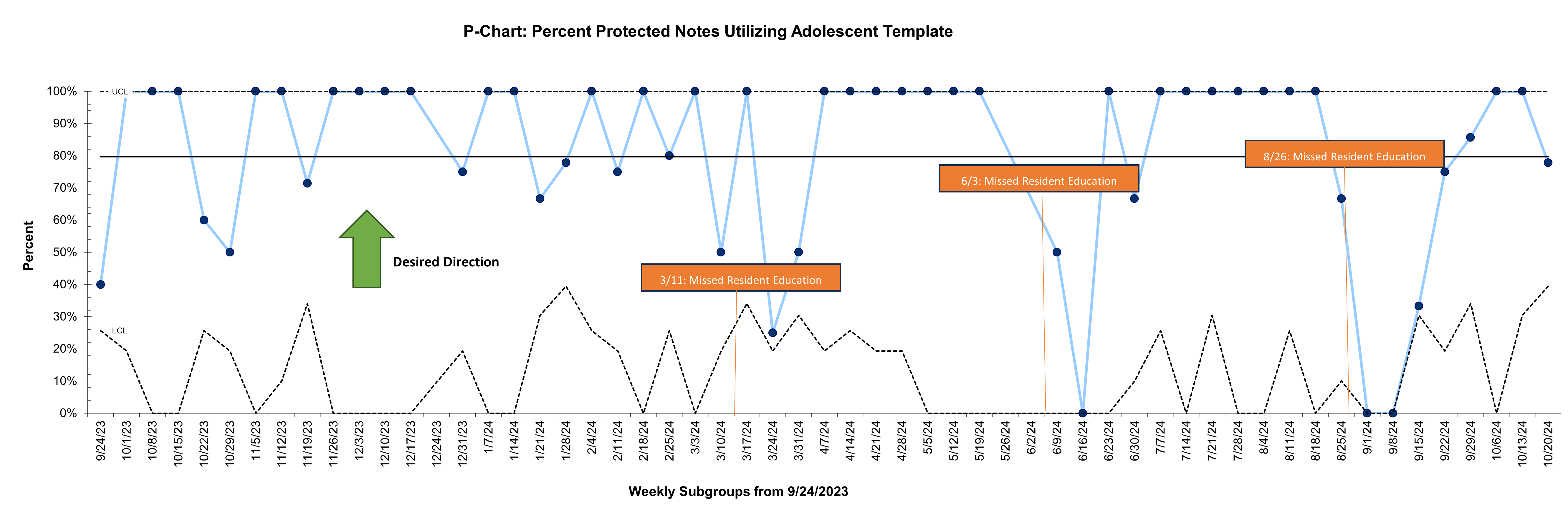 Secondary measure was total separate confidential notes per protected notes after introduction of the separate note template in September 2023. Chart annotations highlight missed resident education sessions.
Secondary measure was total separate confidential notes per protected notes after introduction of the separate note template in September 2023. Chart annotations highlight missed resident education sessions. .png) Process measure was total number of separate confidential notes used per week across all adolescent patient visits. Chart annotations highlight interventions as well as missed resident education sessions. Primary measure was percentage of protected notes for adolescents with a positive suicide screen (Columbia--Suicide Severity Rating Scale). Protected notes included both whole protected notes and separate protected confidential notes. Interventions are annotated. Red dots demarcate notable special cause variation associated with embedding confidential note access in the primary ED note. Secondary measure was total separate confidential notes per protected notes after introduction of the separate note template in September 2023. Chart annotations highlight missed resident education sessions. Process measure was total number of separate confidential notes used per week across all adolescent patient visits. Chart annotations highlight interventions as well as missed resident education sessions.
Process measure was total number of separate confidential notes used per week across all adolescent patient visits. Chart annotations highlight interventions as well as missed resident education sessions. Primary measure was percentage of protected notes for adolescents with a positive suicide screen (Columbia--Suicide Severity Rating Scale). Protected notes included both whole protected notes and separate protected confidential notes. Interventions are annotated. Red dots demarcate notable special cause variation associated with embedding confidential note access in the primary ED note. Secondary measure was total separate confidential notes per protected notes after introduction of the separate note template in September 2023. Chart annotations highlight missed resident education sessions. Process measure was total number of separate confidential notes used per week across all adolescent patient visits. Chart annotations highlight interventions as well as missed resident education sessions. 