
Emergency Medicine 5
Session: Emergency Medicine 5
 photo")
Jake R. Lehman, MD (he/him/his)
Pediatric Resident
Children's Hospital Los Angeles
Los Angeles, California, United States
 Naloxone kits included naloxone, fentanyl test strips, educational materials, and resources for outpatient substance use treatment. Kits were created in English, Spanish, Arabic, Armenian, Chinese, and Korean.
Naloxone kits included naloxone, fentanyl test strips, educational materials, and resources for outpatient substance use treatment. Kits were created in English, Spanish, Arabic, Armenian, Chinese, and Korean.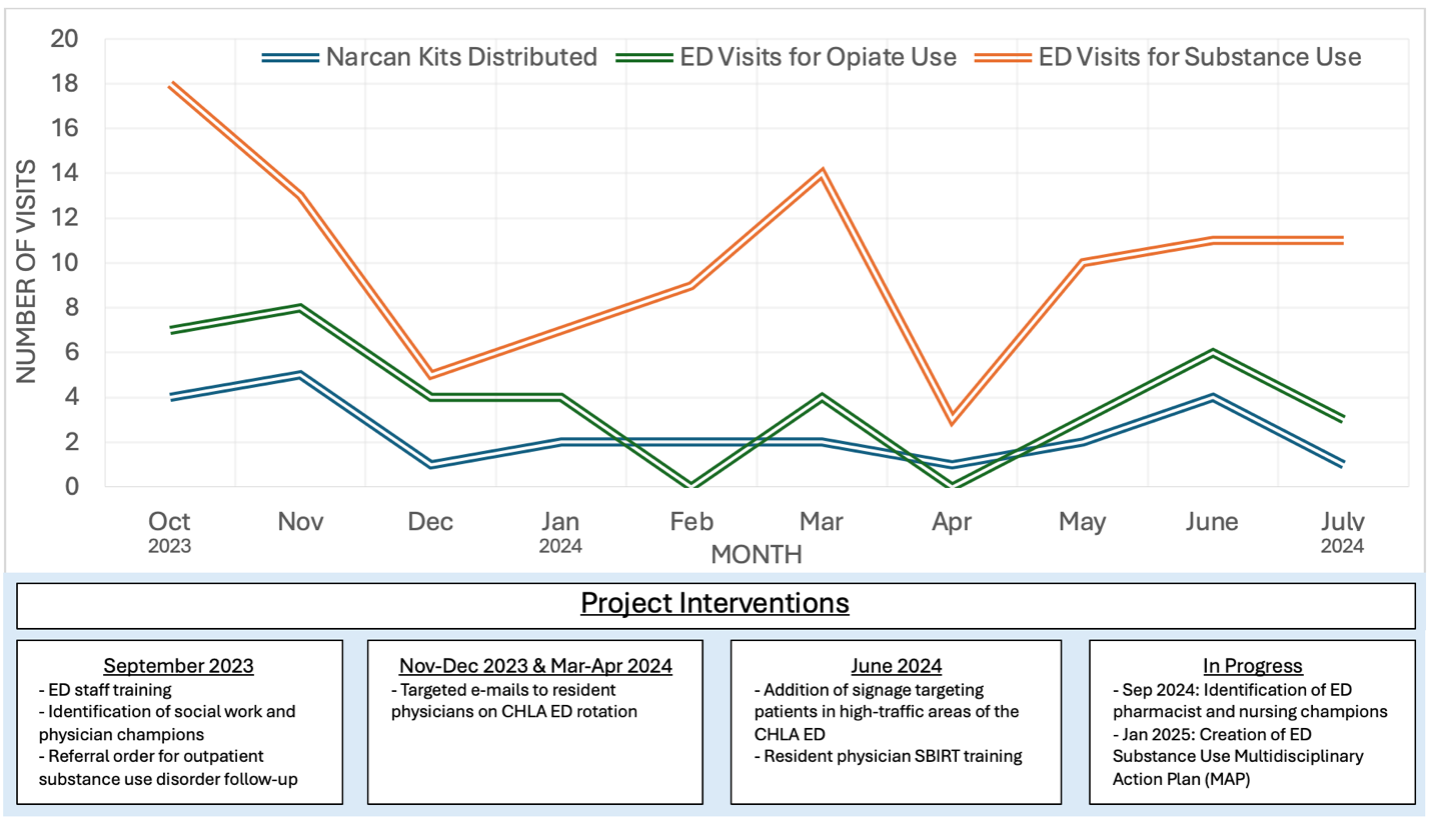 Naloxone kits included naloxone, fentanyl test strips, educational materials, and resources for outpatient substance use treatment. Kits were created in English, Spanish, Arabic, Armenian, Chinese, and Korean.
Naloxone kits included naloxone, fentanyl test strips, educational materials, and resources for outpatient substance use treatment. Kits were created in English, Spanish, Arabic, Armenian, Chinese, and Korean.