
Emergency Medicine 6
Session: Emergency Medicine 6
.jpg "Janine P. Amirault, MD (she/her/hers) photo")
Janine P. Amirault, MD (she/her/hers)
Fellow
Boston Children's Hospital
Cambridge, Massachusetts, United States
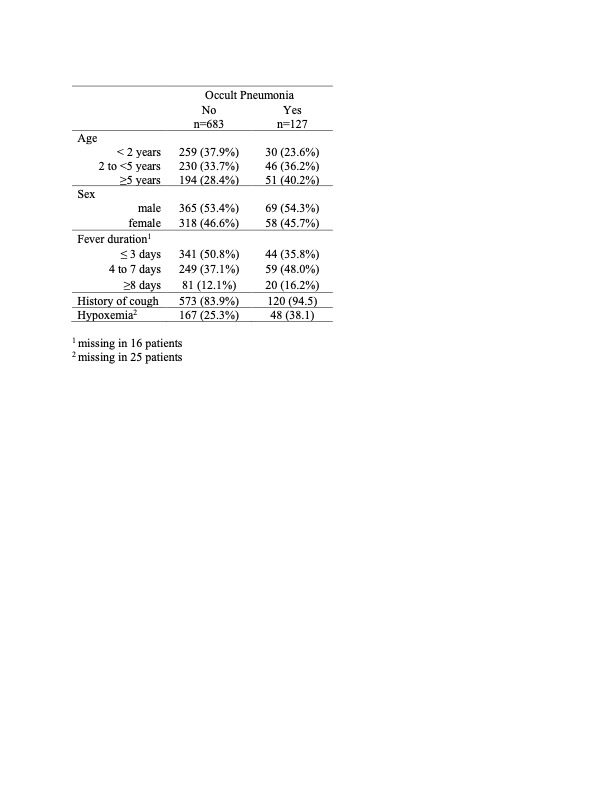
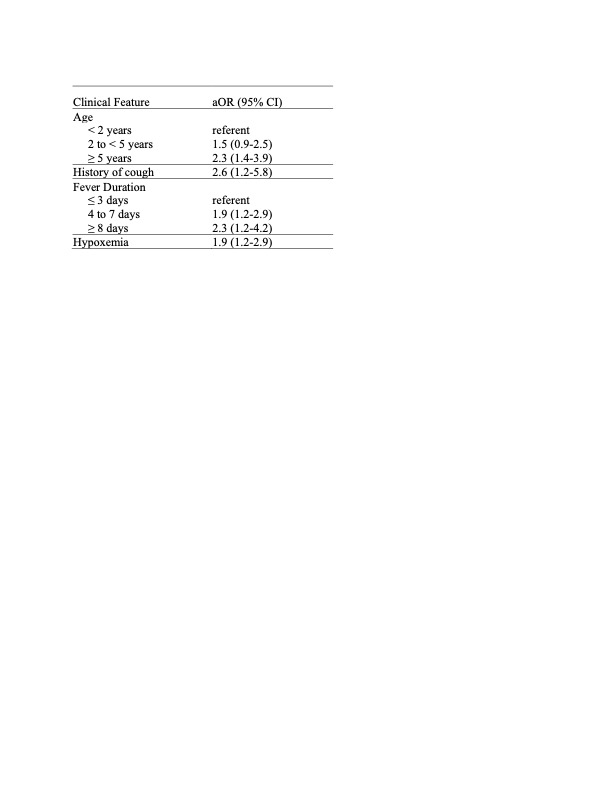 Analysis excluded 40 patients with missing data for oxygen saturation, duration of fever, or both.
Analysis excluded 40 patients with missing data for oxygen saturation, duration of fever, or both.