Neonatal Nephrology/AKI 2
Session: Neonatal Nephrology/AKI 2
Amanda Dyson, MBBCh FRACP MMed (Clin Epi) CCPU (she/her/hers)
Neonatologist
The Canberra Hospital
canberra, Australian Capital Territory, Australia
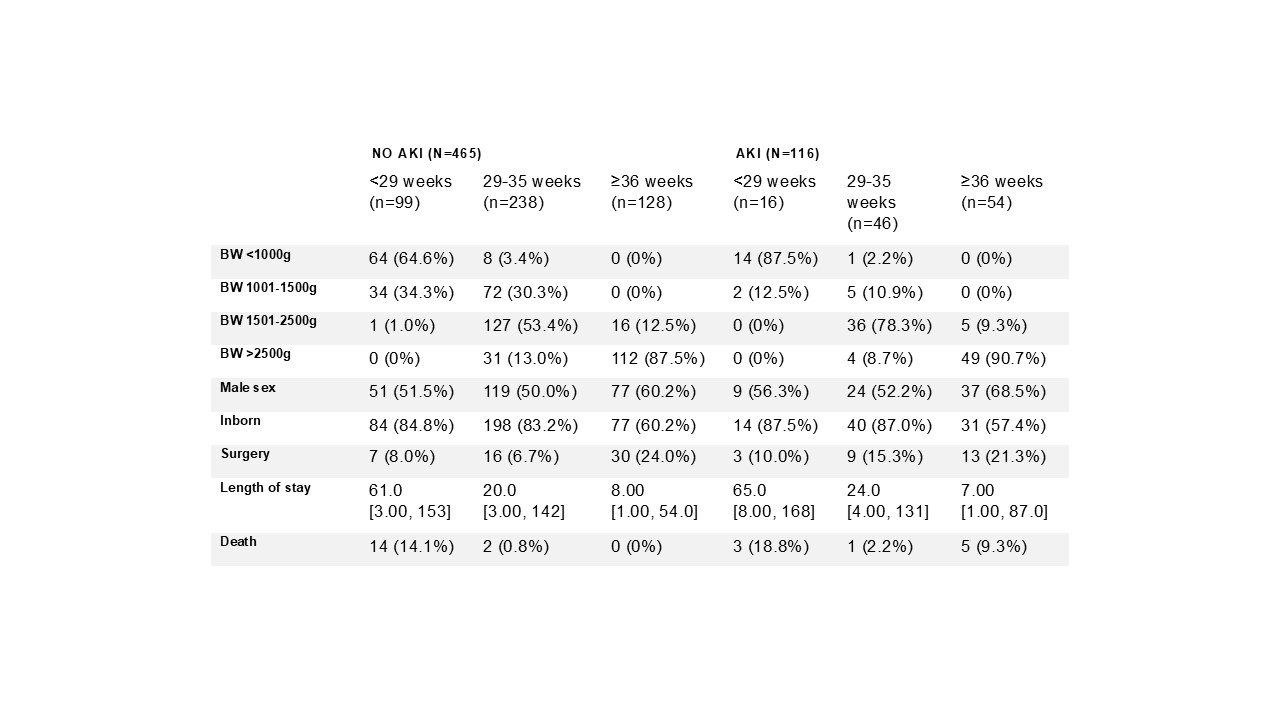 BW: birth weight. Numbers are n with percent in brackets, or median with range in brackets.
BW: birth weight. Numbers are n with percent in brackets, or median with range in brackets.