
Hospital Medicine 1: Quality Improvement
Session: Hospital Medicine 1: Quality Improvement
 Credit")
 photo")
Michelle Noelck, MD (she/her/hers)
Professor of Pediatrics
Oregon Health and Science University
Portland, Oregon, United States
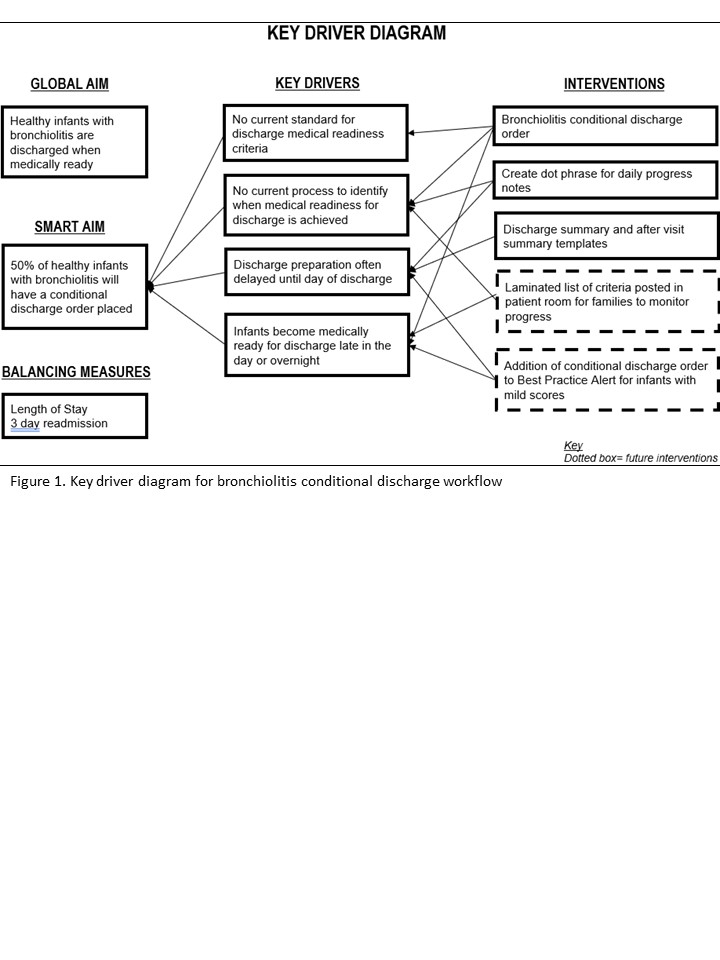 Key driver diagram for the bronchiolitis conditional discharge workflow
Key driver diagram for the bronchiolitis conditional discharge workflow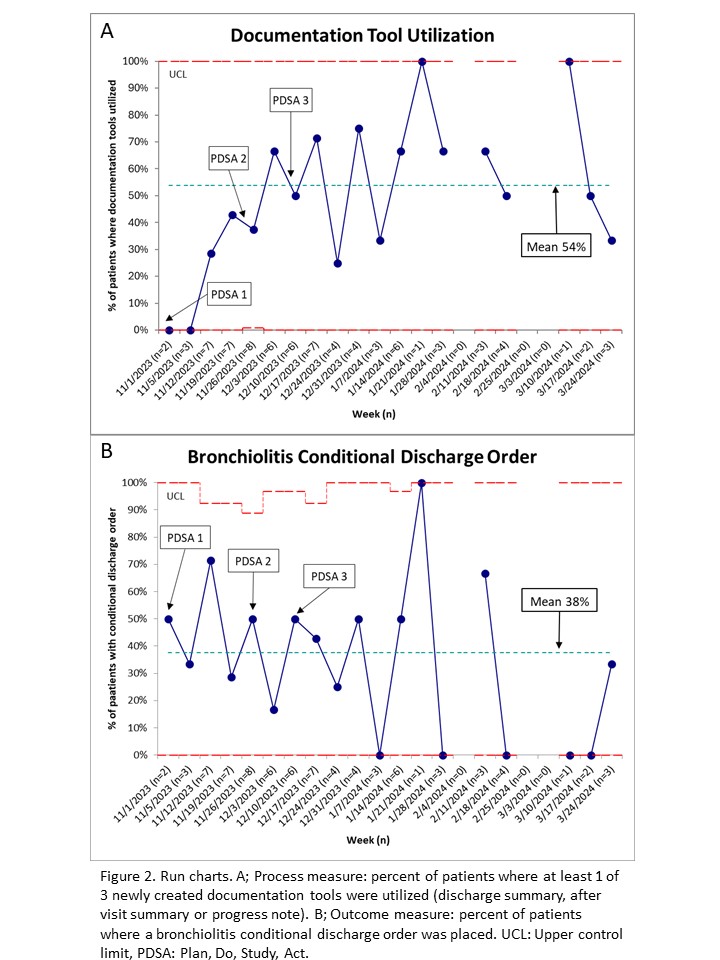 Run charts. A; Process measure: percent of patients where at least 1 of 3 newly created documentation tools were utilized (discharge summary, after visit summary or progress note). B; Outcome measure: percent of patients where a bronchiolitis conditional discharge order was placed. UCL: Upper control limit, PDSA: Plan, Do, Study, Act.
Run charts. A; Process measure: percent of patients where at least 1 of 3 newly created documentation tools were utilized (discharge summary, after visit summary or progress note). B; Outcome measure: percent of patients where a bronchiolitis conditional discharge order was placed. UCL: Upper control limit, PDSA: Plan, Do, Study, Act.