
Neonatal Nephrology/AKI 2
Session: Neonatal Nephrology/AKI 2
 photo")
Thomas A. Forbes, MBBS FRACP PhD (he/him/his)
Paediatric Nephrologist
Murdoch Children's Research Institute
Melbourne, Victoria, Australia
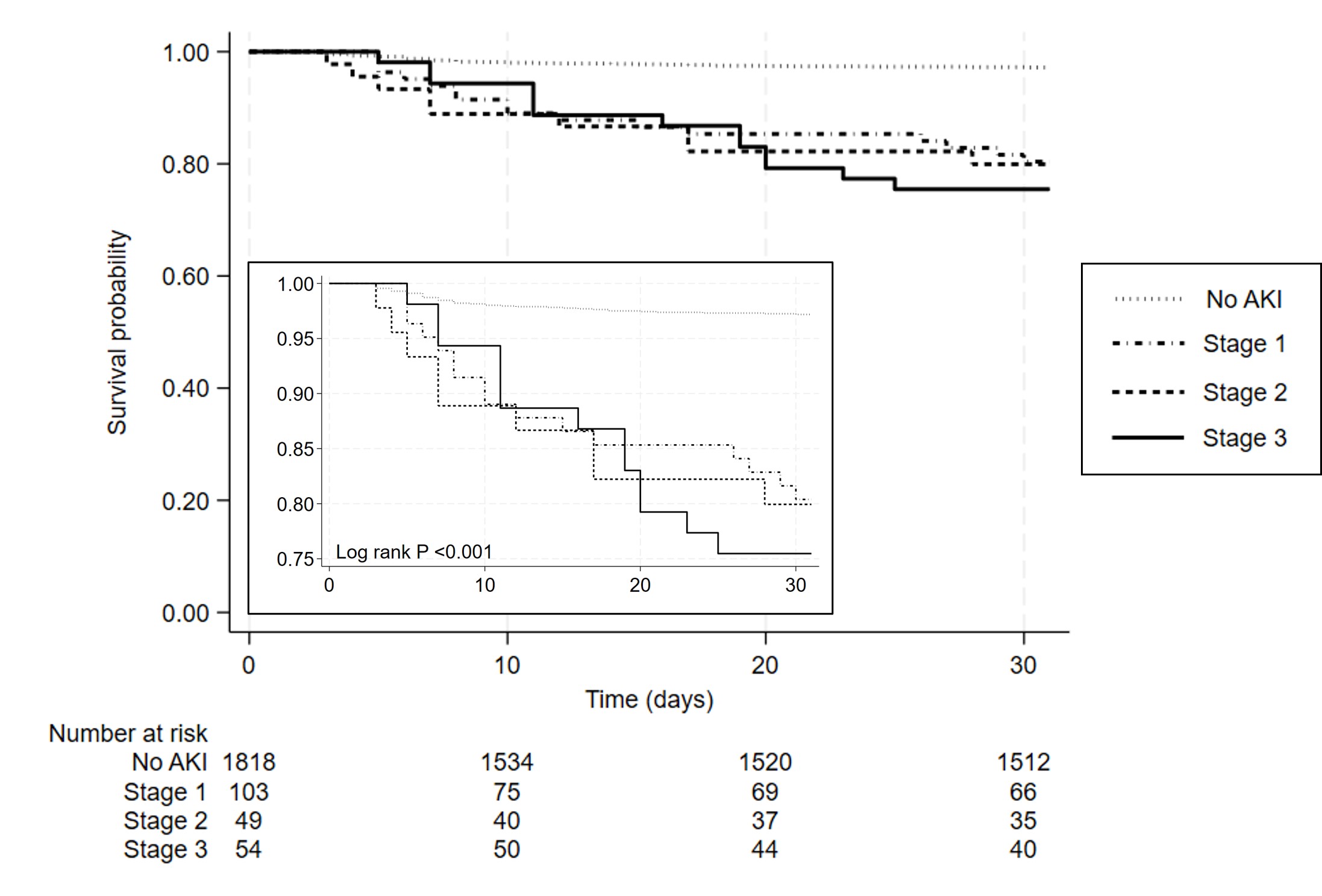 Survival curve for 30 day mortality in 2024 neonates admitted to a quaternary referral NICU according to AKI Stage by modified neonatal KDIGO (creatinine-based only) definition.
Survival curve for 30 day mortality in 2024 neonates admitted to a quaternary referral NICU according to AKI Stage by modified neonatal KDIGO (creatinine-based only) definition. 